|
Site map
Home
Reviews of other ER books
Contact me
Submit a question
Submit an ER story
Have an interesting ER story?
If I use it, I'll give you a free book.
Question & Answer pages
For more Q & A, see my
www.er-doctor.com site
ER crossword puzzle
Interview with Dr.
Pezzi
ER-MCAT
Test your
knowledge of ER terms by solving my ER crossword puzzle that was featured in the
Prudential Securities Healthcare Group 2002 calendar. Or take the ER-MCAT
to see if you have what it takes to be an ER physician.
My favorite
ER memories
Pictures of me
Biography
My personal pages
Including my:
Medical Inventions page
Misc. Inventions page
Snowmobile page
Accelerometer page
Smart Seat page
"If I had a hammer" page
"Sheds I've Built" page
Dremel bit holders page

ER
stuff
A mold to make ER cookies and ER Jell-O! Or
how about a glow-in-the-dark chest x-ray?
My
postings on ER forums
ER links
Bad news about Accutane
Amy's Corner
Amy reviews ER computer games
Tell a friend about this page by e-mail

Recent magazine
interviews

Some of my other sites
| |

Questions about
love and sexual attraction, libido, pleasure, and performance
Have
a question for
Dr. Pezzi? He will be happy to answer it in this forum for free.
And now for the requisite fine print . . .
. All submissions become the irrevocable property of Kevin Pezzi, MD and may be
published on this site in its Q & A forums or in other venues. By
submitting a question, you specify that you are over the age of 18, or have
obtained the approval of your parents or legal guardians and they agree to the
foregoing terms.
No liability is assumed with respect to the use
of the information herein or otherwise provided.
Medicine is an ever-changing science.
The information presented is based upon my assessment of the current body
of knowledge, but this base of information will change in the future.
Hence, before instituting any of the measures presented you should
consult with, and obtain the approval of, your physician for the most current
recommendations. No material
intended for the general population can attempt to treat specific individuals,
and no material in this site or otherwise transmitted to you should be construed
as offering individual medical advice. Given
the innate variability of people, it is critical that your physician approves
the adoption of any information as being safe and effective for you.
A physician's circumspection is his—and your—greatest asset.
 Note: I have all this material on a separate web
site ( www.sexualtips.net
) that is more
extensive and more visually appealing — and the pages load much faster!
:-) Note: I have all this material on a separate web
site ( www.sexualtips.net
) that is more
extensive and more visually appealing — and the pages load much faster!
:-)
Exercise
+ breast discharge = ?
Q: I'm a 29-year-old
healthy woman who began jogging five months ago. Since I began jogging,
I've noticed that my libido has diminished and occasionally my breasts have a
slight milky discharge. Does this make any sense to
you? I thought exercise was supposed to increase libido, if
anything. My doctor is stumped. I'd be very grateful if you can help
me. Thanks, Melissa.
A: It sounds as if you're suffering from a condition called benign
galactorrhea. I will explain this so that it is easy to understand, so
don't be fazed by the big medical words. Galactorrhea
just refers to a condition in which breasts make and discharge milk
at a time not associated with either childbirth or the nursing of an
infant. Benign, of course, simply means that it isn't dangerous.
However, it is a good idea for anyone with this problem to see a doctor for
testing because certain medical conditions can predispose people to galactorrhea,
and these conditions should be excluded before one assumes the condition is
benign.
Your galactorrhea is probably induced by the nipple stimulation that
results from the to and fro motion of your breasts rubbing against your
bra. As I mentioned in
The Science of Sex, nipple stimulation in both
women and men increases the production of prolactin, a hormone that stimulates
lactation (milk production). One of the side effects of prolactin is its
ability to impair libido even if its concentration is not high enough to induce
lactation. Therefore, even people without lactation may be suffering from
the libido-suppressing effects of prolactin. Obviously, for some people
nipple stimulation increases libido instead of decreasing it. The reason
for this is because breast stimulation also increases the release of oxytocin, a
hormone that improves sex in many ways. I'll discuss oxytocin in more
detail at the end of this topic.
It is interesting to look at the connection between nipple stimulation and
libido suppression from a teleological perspective. In other words, did
Mother Nature or God have some logical reason for suppressing libido after
childbirth? Of course! Pregnancy can be very hard on women, and that
was probably more true eons ago before the advent of modern medicine and an
assured food supply. If a woman with marginal deficiencies of some
nutrients became pregnant, the fetus would further sap her. After
pregnancy came lactation (no formula in the Stone Age, obviously), which really
drains energy and nutrients from women. After that, another pregnancy
following shortly thereafter could have been fatal, for the mother, her fetus,
and her infant. Since there weren't any doctors around in those days to
warn women of this serious risk, Mother Nature stepped in and shut down
libido. In case an amorous caveman was able to seduce a woman who was
still breastfeeding, the chance of conception was rather low because the
hormonal changes associated with breastfeeding reduce the risk of pregnancy.
There are numerous causes of hyperprolactinemia (increased blood
prolactin) besides jogging and breastfeeding, including eating, stress,
strenuous exercise of any sort, alcohol consumption, exposure to xenoestrogens
(man-made chemicals that mimic natural estrogens),
certain drugs (oral contraceptives, estrogen, Aldomet®,
opiates, tricyclic antidepressants, phenothiazines, Reglan®,
Compazine®, Phenergan®,
Tagamet®, Prozac®,
and Haldol®), hypoglycemia, primary
hypothyroidism, and sexual intercourse (in women). Apparently bizarre causes of
hyperprolactinemia are certain chest wall lesions, including neoplasms of the
chest wall, herpes zoster (shingles), and surgical scars or trauma affecting the
chest wall. Since prolactin serves to switch off sexual excitement after orgasm,
anyone who wishes to maximize their potential for multiple orgasms should keep
these factors in mind.
Prolactin output is normally held in check by dopamine, a neurotransmitter that
often declines with aging. Hence, prolactin secretion tends to increase with
age. Lindsey Berkson, an expert on endocrine-disrupting chemicals, stated in her
book Hormone Deception that certain chemicals may either mimic or
indirectly affect prolactin. Incidentally, prolactin can contribute to
obesity since it can stimulate appetite and promote fat storage.
OK, what can you do about this problem?
• Switch to a different form of exercise (e.g., swimming).
• Use a sports bra that minimizes breast motion. It may also be a good
idea to place a large Band-Aid® over each of
your nipples before donning the bra.
• Consider taking an herb, vitamin, or medicine. Here are some things
that help:
Bromocriptine (Parlodel®):
Bromocriptine is a drug that can reduce prolactin secretion. Bromocriptine
can improve libido, especially in people with high prolactin levels, and it may
increase sexual pleasure, too. One of the unique properties of bromocriptine is
its ability to increase sexual desire while postponing ejaculation.
Interestingly, since bromocriptine can reduce prolactin secretion, it can
therefore promote fat loss. However, that should be viewed as an ancillary
benefit and not a primary indication for use of bromocriptine.
Ginseng: Ginseng's reputed aphrodisiac effect has a scientific basis
because ginseng can depress blood prolactin levels. This effect is more
pronounced with repeated use.
Vitamin B6: High doses of vitamin B6
can improve libido by reducing prolactin secretion in both sexes. B6
can also improve the quality and intensity of sexual pleasure in some people who have
poor genital sensation. Vitamin B6 is excreted
within 8 hours after absorption, and thus should be supplied at least every 8
hours. An average dose for these conditions would be 50 mg three times daily.
Taking too much B6 can result in too vivid
dream recall. Doses over 200 mg daily can result in neurological disorders if
taken for several months.
Those are some of the specific therapies for combating the
libido-suppressing effects of prolactin. There are many other general ways
of heightening libido, as I discuss in
The Science of Sex.
More on oxytocin
Oxytocin is a hormone that promotes contractions of the uterus during childbirth, but it is produced at other times as well. Its secretion increases during sex and breast stimulation, and it is triggered by certain emotional stimuli. It has been termed the "cuddle chemical" because it promotes snuggling, pair-bonding, and the desire to please others. This may explain why women are more likely to want to cuddle after sex. Thus, there is some truth in the phrase "making love." Oxytocin stimulates erection, enhances vaginal and uterine contractions during intercourse, and increases sexual sensation before and during orgasm.
Oxytocin was available by prescription as a nasal spray (Syntocinon®), intended to assist initial postpartum milk ejection from a woman's breasts after childbirth, but at the time of this writing it is not available; perhaps a generic version will be offered in the future. Oxytocin has been used cosmetically, too. Apparently unaware of the fact that application of a vacuum could achieve the same effect, some Las Vegas showgirls used to sniff Syntocinon to make their nipples more prominent.
Estrogen enhances sensitivity to oxytocin, and thus women with more estrogen are more likely to experience the positive effects of oxytocin—and perhaps its negative effects, too. According to Theresa Crenshaw, MD, author of
The Alchemy of Love and Lust, oxytocin diminishes the capacity to think, reason, and remember.
Breast stimulation increases oxytocin in both women and men, and this is therefore a more readily available means of sexual enhancement than the administration of Syntocinon. The amount of oxytocin produced by breast stimulation in men and nonpregnant women is less than that which can be administered by a Syntocinon nasal spray, but you will not find many doctors willing to prescribe Syntocinon simply to enhance your sexual pleasure. However, since breast stimulation can also increase prolactin (which suppresses libido), relying upon breast stimulation to enhance sex is problematic. Since the ratio of oxytocin to prolactin produced as a result of breast stimulation is individually variable, breast stimulation is not a surefire catalyst for sexual pleasure.
Premenopausal women sometimes become attached to a man with whom they have had sex, even if the man isn't good for them, because the sexually induced secretion of oxytocin encourages this binding. After menopause, intercourse does not result in an oxytocin surge, thus permitting women to make a more rationale, and less instinctive, choice. Premenopausal women who wish to avoid being hormonally blinded should know that alcohol suppresses, and heat increases, oxytocin release. To put this into proper perspective, let's look at some real-world examples.
In women, alcohol temporarily increases testosterone and, hence, libido. However, since alcohol also suppresses oxytocin, women who consume it are more likely to engage in sex, but less likely to feel good about it afterwards. They're also less apt to feel attached to the man, and less likely to feel as if they're falling in love.
Physiologically-hip, conniving men can to some degree circumvent this stumbling block by remembering the effect of heat. Lounging in a hot tub, and then cuddling in a warm bed—or, better yet, vacationing on a warm, exotic island . . . they don't have anything to do with romance and love, do they? Yes, they do, and I think that most people have an intuitive understanding of this.
Women often assume that men desire sex just for the physical pleasure it provides. No doubt, that's sometimes all the man is after. However, I think that many men realize that intercourse can make the woman feel attached to the man. Longing for love, men may desire sex as a means of fostering a romantic bond.
Situational beauty
phenomenon
Q: I'm
not having much luck attracting men. I keep myself in good shape, but I
wasn't born with good looks. I'm not a dog, either, but I'm evidently not
what men are looking for. Short of plastic surgery or new clothes (I've
tried the latter, with no success), what can I do? Thanks for any help you
can give me! Terri.
A: In The
Science of Sex , I devoted one
chapter to the enhancement of intersexual attraction. I put a couple of my
tips elsewhere on my web site, so I won't repeat that info here but I'll provide
a link to that page. One thing that I didn't
mention in my book or on that other web page is that you can enhance your
desirability by taking advantage of the situational beauty
phenomenon. I'll illustrate that by the following story.
A few years ago my brother Ray and I were snowmobiling in Michigan's Upper
Peninsula, and we stopped into a restaurant to get a hot chocolate. A few
minutes later a woman who'd been snowmobiling entered the restaurant, and we
both opined that she was quite attractive. Musing about this over the next
few days, I questioned why we thought that woman was so attractive. She
was slim, but otherwise possessed no extraordinary physical traits.
Moreover, had I passed by her in a mall or in a restaurant in a non-snowmobiling
area, I wouldn't have given her a second look. So what was it about her
that elevated my perception of her attractiveness? The fact that she was a
female snowmobiler. While women who snowmobile aren't quite as rare
as a dodo bird, they're rare enough to stand out in a crowd. I suppose it
is also human nature to reflexively like people who share your interests.
Besides snowmobiling, another activity you might want to try is target shooting
at a shooting range. (Before you non-shooters start guffawing, I should
mention that I took a woman friend of mine to a shooting range and in the course
of a few hours her opinion changed from "I hate guns" to enjoying that
activity so much she didn't want to leave the shooting range.) A single
woman who shows up at a shooting range is bound to attract a lot of attention
from men, and if you try that on a Saturday afternoon and don't have a date for
that evening . . . well, then you do need plastic surgery!
If shooting doesn't rate high enough on your PC scale for you to give it a try,
consider golfing, fishing, boating, camping, or any other activity that draws
men. Yes, some women engage in those activities, but they're usually
tagging along with a man. Try doing it stag and you're bound to attract
attention.
Does
size matter?
Q: I've heard a number of opinions on the topic of whether or not penis
size makes a difference. Does it? Thanks, Tom.
A: Yes, it does matter. However, before you jump to any conclusions,
bigger is not necessarily better. "Big" or even
"average" may be too large, while "small" may be just right
for some women. In my experience as a doctor I've
noticed that vaginal size varies greatly — far more than penile size.
Considering only adult non-virginal women, some vaginas were so small that
they'd provide a snug fit for a pencil, while others were so loose that the
thick end of a baseball bat would easily fit inside. Yes, penile size
varies, but not to that degree. Therefore, for any given couple, the size
of the man's penis is less important than the size of the woman's vagina.
This fact is typically given short shrift in our culture. Whenever the
topic of "size" is broached, it is tacitly assumed that the only size
which matters is penile size, while vaginal size is ignored. If it is
politically correct to discuss penile size, it should be acceptable to consider
vaginal size, too. However, while I frequently hear many direct and
indirect discussions of penile size from sex experts, comedians, ad copy
writers, and even on a daytime court TV program, there doesn't seem to be any
commensurate mention of vaginal size. Again, since size does matter and vaginal size is
the greatest variable, it only makes sense to consider the woman's contribution,
too.
Here is another reason to focus more upon vaginal size than penile size:
women have more control over the tightness of their vaginas than men do over the
size of their penises. While penis size can be increased (especially on a
short-term basis, as I explain in my book), vaginal tightness can be
dramatically altered on a long-term basis by doing Kegel's exercises. In women, one of the greatest benefits of Kegel's
exercises — and one that is rarely mentioned — is that the depth of the outer "tight zone" of the vagina can be increased. I've never met a man whose eyes didn't glaze over at the thought of a tight vagina, but such an improvement can benefit women, too. When this zone of the outer vagina is not just tight, but tight and deep, the penis is better able to stimulate the sensitive outer third of the vagina and the G-spot.
Kegel's exercises are able to increase the depth of the tight zone by causing hypertrophy (thickening) of the pubococcygeal muscles, as depicted in the following diagrams:
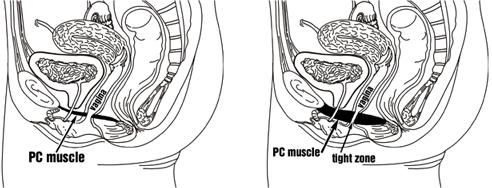
The diagram on the left is from a woman with a poorly developed pubococcygeal
muscle, and the diagram on the right is from a woman with a well-developed pubococcygeal
muscle.
What's
the average size of an adult penis? And why is it less than what it once
was?
Q: Dr. Pezzi, it's Tom again. Thanks for answering my other
question. I showed your answer to my girlfriend, and she now realizes that
"my" problem is "our" problem, and probably even more
"her" problem. But, she's working on it. My question today
is, what is the average size of a penis?
A: The length of an average erect penis in adults is 5.72 inches* (or, if you believe the latest study, 5.1 inches).
Years ago, the average length of an erect penis (measured on the dorsal, or top, surface) was 6½ inches. Later on, it was 6¼ inches, then 6 inches . . . now 5.72 or—gulp—5.1? What's going on here? I hate to tell you this, men, but you are not quite the man your grandfather was; the average penile length is shrinking. Why? There are a number of estrogens (phytoestrogens, xenoestrogens, and exogenous
estrogens**) to which men are now exposed. Furthermore, the estrogen level in men can be increased by a number of factors
(which I discuss in my book in the section on the testosterone to estrogen ratio). Too much estrogen, and the penis either shrinks or fails to grow as much as it should. Not good.
If you're interested, in my book I discuss dozens of environmental factors under
your control that affect penile size.
* As the automobile companies equivocate, your mileage may vary. By random chance, some women have had nothing but large partners, so they may think that a guy with an average-sized penis is small; other women, having only been with men with small penises, may think that an average man is well-endowed. It's all relative. The average erect penis is
1.62 inches wide, and 4.5 inches in circumference. Most men have a penis measuring
4.6 to 6.25 inches long, but 12% of men have larger penises and 12% have smaller penises. Incidentally, the length of a fully stretched flaccid penis is virtually the same as that of a fully erect penis.
** Phytoestrogens are chemicals with estrogen activity that occur naturally in a variety of
plants such as soybeans.
Xenoestrogens are man-made chemicals that mimic natural
estrogens.
Exogenous estrogens are estrogens unintentionally introduced into people from ingestion of food or water containing estrogens from animals, humans, or
pharmaceuticals.
Why did my penis shrink? What can I do about it?
How to trigger a "second puberty" of penile growth
Q: I am writing to you
because my doctor is an idiot. I'll explain why in a minute. I am 47
years old, healthy, have usually one beer each evening, never use drugs, don't
smoke, and I haven't gained any weight. I see my doctor once yearly for an
annual checkup. So far, so good, except for one thing. My penis is
shrinking. It doesn't look as big, or feel as large when I grasp it with
my hand, even when it is fully erect. I mentioned this to my doc, and he told me that penises don't
shrink. Well, mine did. It's about ¾
inch shorter, and ½ inch less in circumference. My doctor thought I
measured wrong. No way. I work as a machinist, and routinely measure
things to an accuracy of less than one-thousandth of an inch. There is no way that my
measurements are wrong. I must have measured my penis at least a dozen
times when I was a teenager, and I've checked it several times in the past few
months. There has been a definite size decrease, so I know my
doctor is just plain wrong about his statement that penises don't shrink.
My questions are: 1) Why did my penis shrink? 2) What can I do about
it? 3) Why do doctors say that penises don't shrink, when they clearly do?
I assume I am not the only man who has experienced this problem.
A: You are not alone. I'll tell you about a 62-year-old patient I
saw in the ER years ago. As I prepared to insert a catheter into his
penis, I asked his daughter to step out of the room. He said, "That's all
right, doc. She can stay in here. There isn't much left to see.
It used to be large, and now it's just a shriveled up noodle. But I'm
proud of what it did. It gave me two beautiful children." This
revelation about the shrinkage piqued my curiosity, and I would sometimes ask
other patients if they had the same problem. Amongst older men, this was
surprisingly common. This caused me to wonder why so many doctors cling to
the belief that penis size is fixed at the end of puberty. I know of a few
cases in which there has been a documented size increase (I discuss why in my
book), and many more cases of shrinkage. Tissue shrinkage is actually a
very common accompaniment of aging. Breasts shrink, the vagina shrinks
(unless estrogen is given after menopause), the brain shrinks, skin and bones
thin, muscles atrophy, lips shrink, testicles shrink, we become shorter, and so on. In spite of this,
physicians routinely maintain that penis size does not change. The penis
of an average 88-year-old man is just as large as it was on his 18th birthday?
Hogwash. Doctors are wrong. Don't be too surprised, though.
This isn't the first medical myth to crumble under the weight of objective
scrutiny. For example, there is the myth that the average body temperature
is 98.6° F. That is not true, but many docs are seemingly ignorant of
circadian temperature variation and research which indicates that the average
body temperature is not 98.6° F. If doctors can be deceived by the
body temperature myth, it is not surprising that they can be duped in regard to
age-related changes in penile size — a far more esoteric subject.
Doctors routinely see men in their flaccid state, rarely inquire into their
erect size, and almost never discuss if there's been any change in size.
With this in mind, I have a difficult time understanding why physicians feel
qualified to make a sweeping generalization that penis size is immutable.
They believe that to be true because they heard it from another doctor, who just
passed on what he heard from another doctor who also didn't know the truth
because he was just relaying a myth that he'd heard or read from someone
similarly uninformed. Is this any way for learned professionals to behave?
Why did your penis shrink? That could result from decreased testosterone
and especially dihydrotestosterone
(DHT), which is derived from testosterone. DHT is known to be the primary
catalyst for penile growth. Physicians are taught in medical school that
this is important only before the end of puberty; once the penis develops, it'll
maintain that size forever. I know that is wrong, and it
frankly doesn't make any physiological sense to me. As I discuss in my
book, the body continuously rebuilds itself. If your house could do the
same thing, it could tear off an old shingle and replace it with a new one.
In time, your house would replace all of its shingles, and you'd have a new
roof. Your body does a fairly good job of renewing itself until you hit
middle age, at which time tissue regeneration begins to sputter. After a
few more decades, this process slows even more. Wounds heal more slowly,
and muscles take longer to regenerate after exercise.
If the cells and molecules in your body were not broken down, you could live off
sugar water. You wouldn't need protein. But you do require
dietary protein and other nutrients because tissue destruction and regeneration
constantly occur. This process is more rapid than you might imagine,
because your body recycles some of its building blocks. Only a fraction of
the recycled material is lost in the urine or feces.
The bottom line is that the vast majority of the molecules in your body weren't
there a year ago. The old ones are gone, and new ones have taken their
place. Even bone, which may seem as active as a fossil, is torn down and
rebuilt. The penis is no exception. Let's think about this
logically. If DHT is critical for stimulating penile growth (and it is),
why would this matter only before the end of puberty? Isn't there still a
receptor for DHT after puberty? Yes, of course. Once DHT
binds to the receptor, doesn't it affect DNA transcription, as it does before
puberty ends? Yes, of course. However, physicians who contend
that penis size is fixed after puberty would have you believe that it doesn't
matter if your DHT level is zero, or if you have DHT bubbling out your ears.
Can you think of any other example in which the level of a hormone is totally
immaterial to its target tissue? I can't. I graduated in the top 1%
of my class in medical school, so I am not ignorant about how the body works.
Hormones exist for one reason: to influence their target tissues.
In reality, the penis becomes less sensitive to DHT after puberty, but the
sensitivity is not zero. Thus, the DHT level can influence penile
size, but to a much smaller degree than it could before the end of puberty, when
the penis was still very sensitive to DHT. As I mentioned before, I don't
think the DHT level matters after puberty in regard to penis size, I
know it. (If any physician or scientist doubts this, put your money
where your mouth is. Let's wager a million dollars. You'll lose.)
After reading all this, you might think that increasing the DHT level is the way
to go. It may help a wee bit, but there is a much better secret that I
accidentally discovered. I discuss this topic in
The Science of Sex. Using
this method, your penis won't just be larger, it will be exquisitely
sensitive, and sex will feel much better. Your libido will increase to the
point that you would be called a nymphomaniac, if you were a woman.
Besides DHT, other factors influence penile size. Genetics obviously
matters, but it is pointless to discuss them because this is not under your
control. In terms of what you can influence, DHT is the most important
factor, but there are others. I won't reiterate everything I said in my
book, but I will briefly mention other things that make a difference:
other hormones, hormone transport proteins such as sex hormone binding globulin
(SHBG) and albumin, cadmium, zinc, antiandrogens, phytoestrogens, exogenous
estrogens, endogenous estrogens, xenoestrogens, obesity, numerous drugs and
chemicals, collagen, elastin, and a dozen other factors.
Why
does sexual pleasure vary so much from one woman to the next?
Q: I'd like your medical opinion on something. I've had sex with
over 60 women and I've noticed that there is a huge difference in the pleasure I
feel during sex with different women. With most of the women it's very
pleasurable, with a few it's so little pleasure it's barely worth doing, and
with some others it is so pleasurable it's off-the-scale, out-of-this-world,
mind-blowing pleasure. Why is that? I used to think that tightness
was the only thing that made any difference, but there's more to it than
that. I don't think that this variation is attributable to how horny I am
because some women are consistently duds and others are consistently
extraordinary. Plus, on a few occasions I've had sex with two women,
changing partners every few minutes, and I know there can be a significant
difference. Why? Another thing I wonder about is why sex feels so
different even amongst women who are extraordinary. I don't know how to
explain this other than to compare it to eating pizza and eating steak. I
love both equally well, but they taste entirely different. So can you see
what I'm trying to say? When I think about the two women who've given me
the most sexual pleasure, the sensations I got from each women was noticeably
different. This really has me stumped. I know there must be some
factors that make one vagina better than another, but how can two vaginas feel
equally fantastic but yet very different? Thanks, Phil
A: You're correct, there is a significant difference. I've noticed
it, and other men have reported to me that they've noticed it, too. There
are many factors that underlie this difference, and I discussed them in a
chapter in The Science of Sex. One of the reasons
why I explained this so extensively is because men sometimes dump women who are
"duds," as you termed them. What's important for women to
realize is that many of the factors that influence this variation in pleasure
are things they can influence.
I don't intend to minimize the importance of love in a relationship, but the
fact is that an average couple in the United States begins having sex after
three dates. I think it is safe to assume that most men are not truly in
love after three dates, so if they don't obtain the pleasure they're seeking
they don't feel compelled to stick with that woman. I've heard many women
wondering aloud, "Why did he dump me right after we slept
together?" Well, it's not because your bedroom was messy, trust
me. Maybe the guy suddenly realized he needed to spend more time mowing
his lawn . . . or maybe he's been spoiled by sleeping with women who gave him
substantially more pleasure. Such pleasure is addicting, and once a man
has experienced it, he will often turn up his nose at women who have less to
offer in the bedroom. My message to women is this: you can't change
the expectations of men, but you don't have to be snubbed. If what you
have isn't good enough for the men in your life, you can make it better.
I'd like for all women to be superstars in that department, because that would
force men to choose partners for more substantial reasons. As a doctor,
I've witnessed the pain experienced by women who are repeatedly rejected after
The Night. Again, women are dumped for other reasons, but this is one, so
why ignore it?
To answer your question about why sexual pleasure can be quantitatively the same
but qualitatively different (i.e., both are equally pleasurable but in different
ways), the primary reason for this is because there are so many factors that
account for the differences in sensation amongst women. As an analogy,
consider the three basic colors (red, blue, and green) that are combined to
produce the spectrum of colors on your computer monitor or television set.
Those three colors can combine to produce equally beautiful but substantially
different colors. Or imagine the different flavors produced by cooks who
combine flour, sugar, butter, and eggs in different ways to produce entirely
different foods. The ingredients may be the same, but when the proportions
are varied the end result can be quite different.
Sign
up for the Sexual Tips newsletter, published monthly.
It's free, and there are no annoying ads.
Your e-mail address will never be disclosed to anyone else.
To begin your subscription, check the appropriate box in the form on this page:
www.myspamsponge.com/doctor.php
Q: While browsing at the bookstore, I came across a book which proclaimed that the cul-de sac is the "ultimate pleasure spot." First, what is the cul-de-sac? Second, is it really the ultimate pleasure spot?
A: The cul-de-sac (also known as the rectouterine pouch or the pouch of
Douglas) is a space above the vaginal apex, above the posterior uterus, and in front of the rectum (see diagram).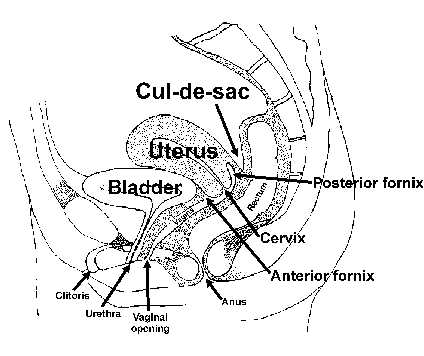
In reality, there is no direct way to stimulate the cul-de-sac during sexual activity. It can be indirectly stimulated by stimulation of the cervix or posterior fornix. The cervix projects down into the vagina near its apex, leaving a circular recess around it called the vaginal
fornix.
So why did that author say that the cul-de-sac is the ultimate pleasure spot? Probably because
cul-de-sac is a sexier and more euphonious term than posterior fornix. Aside from that minor point, is that area some sort of magical hot button? Yes and no. I hate to equivocate, but there's no simple answer. Here are the facts:
• Some women do obtain extra pleasure from cervical stimulation during coitus. If the penis thrusts deep enough to contact the area around the posterior fornix and cul-de-sac, it will inevitably contact the cervix, too. Since these structures are in a small area and they're attached to each other, stimulating one will stimulate the others. Hence, it's a moot point whether one area is the "pleasure spot."
• Calling it the ultimate pleasure spot is a bit of an overstatement. Most women think that the ultimate pleasure spot is the clitoris, especially when the clitoris is stimulated along with the outer vagina and G-spot. Think of that as the South Pole of Pleasure, and the cervix, posterior fornix, and cul-de-sac as the North Pole of Pleasure. Which is the ultimate pleasure spot? 99% of women would choose the South Pole any day — or night.
• For some women, the North Pole isn't the ultimate pleasure spot, it is the ultimate
pain spot. If a woman has endometriosis* or an infection of her cervix or tubes, deep thrusting can be uncomfortable or even exquisitely painful.
* A condition in which functional endometrial tissue is present outside the uterus (the endometrium is the lining of the uterus).
Do
I have a fornix?
Q: Hi Dr. Pezzi. I've just discovered your question & answer page
and have found the reading very interesting. I was doing a search trying
to find a diagram of the cul-de-sac after reading about it in a book entitled
Super Sexual Orgasm. I found your diagram and description, however now
I'm concerned that I may not even have a posterior fornix after a total
hysterectomy. Am I correct in assuming this? Thanks for your
information, Alexandra.
A: By definition, the vaginal fornix is the recess or arch (fornix
is a Latin word that means "arch") formed between the vaginal wall and the part
of the cervix that projects into the vagina. If you've had a total
hysterectomy that removed your cervix, you do not have a posterior fornix (or an
anterior fornix, for that matter). I wouldn't fret over this for a couple
of reasons. First, some of the tissue that once formed your fornices
(plural of fornix) is likely still present, but instead of reflecting or looping
into an arch-like structure, it is just sewn together into what is sometimes
termed a "blind pouch" that forms the end of your vagina. Secondly, I
don't know of any evidence which suggests that the fornix tissue possesses any
special sexual properties. Some of the magic attributed to it is instead
due to the cervix. However, as I've pointed out before, not all women
think that cervical stimulation is pleasurable. Some love it, some think
it feels "weird," while others think it is downright painful (although these
latter women usually have some sort of pelvic pathology).
Doctors are now — thank God — less cavalier about hysterectomies than
they once were, so if your doctor removed your uterus and its cervix, he likely
had a good reason for doing that and you are probably better off without them.
"I
don't get horny any more"
Doctors think that "OK is good enough," but patients don't
Q: I'm a 36-year-old married man with a problem. I'm healthy and I
don't smoke or use drugs, and I rarely drink. I'm happy, except for one
thing. I don't get horny any more. I still have sex, but that's
primarily because I want to please my wife. I never have that burning
desire for sex that I once had. When I do have sex, it feels OK, but it's
not as intensely pleasurable as it once was. I saw my doctor about this,
and since I can still get an erection, have sex and an orgasm, he didn't see
what the problem is. He just doesn't get it. Is there hope
for me, or should I just give up? Steve
A: Yes, there is hope for you. First, let me tell you a little
secret about doctors and their modus operandi when confronted with a
problem for which they're clueless. Doctors don't like to concede a lack
of knowledge, so rather than admit that they cannot solve a problem, they'll
trivialize it. If the problem is sufficiently minimized, there's no
problem to be solved (at least in their minds), so this mitigates their anxiety
about not knowing the answer to the problem. This psychological defense
mechanism doesn't just afflict quacks who work in seedy offices; I know
physicians who are members of the faculty at the most prestigious medical
schools in the world, and they do it, too. When they don't have an answer,
they pull this dismissive stunt. Furthermore, in subsequent private
conversations with their colleagues, they'll often denigrate both the problem
and the patient.
That's enough psychological dissection of doctors and how they respond to a
potential threat to their egos. Now, on to your problem. I'm amazed
that so many doctors simplistically assume that erection and orgasm are evidence
that everything is A-OK in that department. There are erections, and there
are rock-hard, fully inflated erections. In terms of preorgasmic and
orgasmic sexual pleasure, there is pleasure, and there is pleasurable that is
indescribably intense. The realization that pleasure varies so much was
one of the primary factors that spurred my interest in researching sex, because
this topic has been given short shrift by the medical profession. Ask a
typical gynecologist or urologist why some women can give men more sexual
pleasure during intercourse. The traditional medical view is that this is
explained by one variable, vaginal tightness. If you want to be
entertained, you might try this some time: press the doc for more reasons
why this variation exists. Most likely, he will hem and haw, say "um,"
scratch his head, and look befuddled. Ask him to enumerate a half-dozen
reasons, and he'd be utterly stumped. This is one of the central flaws of
medicine. Doctors assume that the absence of disease is health, and
pleasure is pleasure. Obviously, things aren't so black and white.
People don't just want to be free from disease, they want to have radiant health
and feel great. They don't want just so-so sexual pleasure, they
want intense sexual pleasure. However, physicians possess a
different mindset, and they think that "OK is good enough." This
conviction pervades most specialties within medicine (with the notable exception
of plastic surgery, where there is a relentless pursuit of "even better").
Hence, I am not surprised by the apathy evinced by your physician when you
discussed your problem with him. The good news for you is that there are
many causes of diminished libido and sexual pleasure that are easily treatable.
I can't discuss every possible cause in this space, but here are a few that I
will briefly mention. Your testosterone level may be low, or your estrogen
level may be too high, thus depressing your testosterone-to-estrogen ratio.
You may have too much SHBG (sex hormone binding globulin), a blood protein that
gloms onto testosterone to transport it, but in the process makes the
testosterone inactive. You may have another hormonal imbalance, even
endocrine problems that seemingly have
nothing to do with sex. You may be deficient in some nutrient, or
you may be suffering from an exposure to some chemical in the environment.
Surprisingly, common chemicals that people are exposed to every day have
the potential to rob them of sexual gratification. As strange as this may
sound, the problem may not be you, but your wife. Apart from the obvious
(e.g., is your wife still attractive and loving?), there are several
physiological reasons why your libido hinges not just on you, but also what goes
on in your wife's body. I explain all these things, and many more, in my
book.
Accutane causing vaginal pain and fragility
Q: When I took my second course of Accutane I developed severe vaginal
pain during intercourse. For two days following intercourse, my vaginal
lining would slough and during this period of time it was extremely sore.
No tampons could be inserted and certainly no penises either! I saw
several doctors through Kaiser Permanente, but none knew why it happened.
Not one of them linked it to Accutane. It became almost impossible for me
to have sex. I could still do it for a minute or two with a bearable
amount of pain, but that too became rare. It has gotten to where I cannot
have intercourse at all as insertion of anything feels like I am being stuffed
with an extra large sandpaper dildo. Of course, this reduced my appetite
for sex. I was a beautiful, flirtatious young lady with a steady boyfriend
when this happened to me and suddenly my hopes for a healthy sex life or even a
marriage were more or less destroyed.
Have you read about the researcher who worked for Roche who claims that
Roche ordered him to destroy research documents on Accutane? I may have a
copy of his story if you're interested. Niki
A: Yes, I am very interested, and I'd greatly appreciate that.
I think I will be able to help you overcome your problem, or at least
minimize it. First, some background information. Accutane is known
to cause skin fragility and dryness. It can also cause dryness of the
mouth, lips, eyes, and nose. It can cause peeling of the palms and soles.
It can induce eyelid inflammation and conjunctivitis, which is inflammation of
the conjunctiva (the mucous membrane lining of the inner surface of the eyelid
and the exposed whitish surface of the eyeball). It increases the
probability of epistaxis (nosebleed). It can trigger keratitis
(inflammation of the cornea). It can cause inflammatory bowel disease.
It can also cause bleeding and inflammation of the gums (an interesting aside
that is tangentially related to Accutane: researchers discovered that gums
undergo cyclic hormonal changes during the menstrual cycle, which led them to
theorize that oral tissues, like the vagina, possess hormone receptors).
Considering the foregoing, I am not surprised when I've heard women report
problems similar to yours. Accutane causes many problems other than the
ones listed above, but one of its characteristic effects is to cause
abnormalities with skin and mucous membranes (a.k.a., mucosa). The vaginal
mucosa is not an exception, as you know.
In the Physicians' Desk Reference, Roche admits that the "exact
mechanism of action of Accutane is unknown." Hence, it is not surprising
that they do not understand the causation of Accutane's side effects. I
think some of Accutane's effects result from it interfering with the action of
certain hormones. This plausibly explains why Accutane can decimate libido
and sexual pleasure, and why it can lead to vaginal problems such as yours
(fragility and pain) that are typically seen only in hormonally deficient
postmenopausal women. Hence, one logical therapeutic option is to use
supplementary hormones. The mechanisms by which hormones act are very
complex. Many doctors oversimplify this subject and think, or act, as if
hormone levels were the only important key. In reality, they are just one
link in the chain that begins with the body trying to do something and ends with
the body accomplishing that task. Hormonal effects can be blocked by
competitive inhibition (which I explain in
The Science of Sex), various
nutritional deficiencies, genetic problems, and exposure to certain chemicals —
including Accutane, in my opinion.
I will give you an analogy to help illustrate why measuring hormone
levels will not necessarily ensure that your hormonal effects are OK.
To clarify this, I'll put the analogy equivalents in parentheses. Let's
say that someone (a patient) has difficulty hearing sound (achieving a hormonal
effect) from his AM radio (body). He consults an engineer (doctor), who
uses a signal strength meter (a lab test) to determine the strength of the radio
waves (the hormone level) in that area (in that patient). If you're
knowledgeable about electronics, you know that the engineer could not possibly
declare that everything was OK just because the signal strength was fine.
Perhaps the radio receiver (the hormone receptor) was defective or blocked.
Do you see what I'm getting at? Hormones do nothing by themselves.
They're just messengers the body uses to signal desired effects.
Just because the signal is OK does not mean the effect is OK.
Inexplicably and perversely, many physicians ignore this fact. Whenever
they wish to gauge action of a hormone, they do a lab test to measure its level.
If engineers were that illogical, they would measure AM radio sound levels by
testing radio wave signal strength. If you found an engineer that daffy,
you'd fire him and find someone else.
I am not opposed to measuring hormone levels, but it is important to
remember that hormone levels are just one link in the chain, so to speak.
It is also important to assess the hormonal effects. If I were your
doctor, I would evaluate the adequacy of your hormonal effects by looking at the
hormonally responsive tissues of the body. Some of this investigation
would involve visual clinical judgments, while other facets of the evaluation
would involve biometric assessments and microscopic evaluations of
hormone-responsive tissues (such as vaginal cells). I'd also use various
clues (e.g., old photos and your self-assessments, pre- and post-Accutane) to
help determine if Accutane is indeed blocking some of your hormonal effects.
I'd then consider the totality of the evidence from your history, physical, and
lab tests to assess whether or not your body's hormonal messages are "getting
through," so to speak. I would not tell you that everything was hunky-dory
just because your hormone levels were OK. If your hormonal effect deficits
were confined to your vagina, you and I would consider using a topical vaginal
cream to supplement the local hormonal effects. If your problems were more
widespread, we might opt for oral or transdermal hormonal supplements.
But what if hormonal effects were not the root cause of your problem?
Some of Accutane's adverse effects have no clear-cut connection with hormones.
If that were true in your case, I'd offer you an invention I conceived while
reading your question. This would enable you to experience pleasure with
intercourse, instead of pain, and it would also be pleasurable for your partner.
I assume that simple measures, such as sexual lubricants, were not adequately
helpful.
If you want to read my book The Science of Sex, let me know and I
will give you a free e-book copy of it. In any event, let's keep in touch
and solve your problem.
The next two Q&A topics generated some heated
debate from people who mistakenly assumed that I said it is impossible to
contract an HIV infection through vaginal intercourse. I never said that. I
have no doubt that it can spread that way because cuts, tears, and
abrasions may develop in the vagina. A man may develop similar epithelial
defects, or also pass HIV through his semen. While it is possible to
transmit HIV via vaginal intercourse, I think the risk of this has been
overemphasized in the press, and the risk of dying from other diseases has
been underemphasized.
To illustrate this, let’s look at data from
the CDC’s National Vital Statistics Reports. For 1999, the most recent year
for which final data are available (I have no idea why the government takes so
long to finalize their data), death from HIV is not even in the top ten list
for all races, sexes, and ages. What is in that list? Heart disease,
malignant neoplasms, cerebrovascular diseases, chronic lower respiratory
diseases, accidents (unintentional injuries), diabetes mellitus, influenza and
pneumonia, Alzheimer’s disease, nephritis, nephrotic syndrome, nephrosis, and
septicemia. Have you ever heard the general press discuss nephritis, the
nephrotic syndrome, or nephrosis? Have you ever heard a scary public service
message about these diseases? (Do you even know what they are?) Do
somber Hollywood celebrities ever give you stern warnings about them? Or what
about septicemia? I’ve never heard any such message, yet I’ve heard thousands
about HIV. Now can you understand why I used the words overemphasized
and underemphasized?
HIV shows up in the top ten lists only when
deaths are categorized by age. Even then, the statistics show results that
may surprise you if you obtain your information from the mainstream media.
People in the 20 to 24 age group were 83 times less likely to die from HIV
than from greater threats (accidents, assaults, suicide, malignant neoplasms,
heart disease, congenital malformations, and chromosomal abnormalities).
People in the 25 to 34 age group were over 10 times less likely to die from
HIV than from greater threats (accidents, suicide, assault, malignant
neoplasms, and heart disease). Imagine that! Even in such young people,
cancer and heart disease (often thought to be primarily diseases of the
elderly) are bigger killers than HIV. People in the 35 to 44 age group were
over 8 times less likely to die from HIV than from greater threats (malignant
neoplasms, accidents, heart disease, and suicide). People in the 45 to 54 age
group were almost 30 times less likely to die from HIV than from greater
threats (malignant neoplasms, heart disease, accidents, chronic liver disease
and cirrhosis, cerebrovascular diseases, suicide, and diabetes mellitus). In
other age groups, HIV did not make the top ten lists. Combining data for
people aged 20 to 54 reveals an interesting statistic: those people are 16
times less likely to die from HIV than from another cause — some of which
you may never have heard of. Furthermore, this group includes homosexuals,
drug abusers, and heterosexuals who engage in anal intercourse. It also
includes countless heterosexuals who don’t use drugs or have anal sex, but
aren’t very choosy about selecting sexual partners.
There is no doubt that HIV stirs up quite an
emotional reaction in some people, but for a moment I’d like to ask you to
dispassionately consider this matter. If you do that, you cannot help but
face the fact that you’re far less likely to die of HIV than you are of
something else. This is true even if you bend over backwards to look at the
most gloomy statistics and consider only the high-risk age groups and don’t
separate out homosexuals, drug abusers, or heterosexuals who engage in risky
behavior (anal sex, or being cavalier in regard to partner selection). If you
do omit those groups, the risk is considerably less.
I’ve read all sorts of statistical analyses of
the death risk for heterosexuals who don’t abuse drugs, don’t have anal sex,
and are prudent in partner selection. The figures show that those folks are
hundreds to thousands of times less likely to die of HIV than from other
causes. Even if you insist on looking at only the highest-risk age groups and
don’t omit the people who engage in risky behavior, the risk of death from
something other than HIV is about 94%. From this, I think that any
fair-minded person would have to conclude that HIV has indeed been
overemphasized. Thousands of public service commercials about HIV and
none about some diseases that are bigger killers, yet are unknown to
the average American? Is this balanced? Obviously not.
Should
heterosexuals worry about AIDS? Why did the media lie about this?
(If you haven't already read the above text in
the yellow box, please do so now.)
Q: I just heard an
interview with Bernard Goldberg, a respected journalist who had a long career
with CBS. He wrote a book entitled Bias: A CBS Insider Exposes How the
Media Distorts the News. In this interview he said that the media
distorted the facts about AIDS as it pertains to heterosexuals. Basically,
he said that the media made it seem like any heterosexual could get AIDS from
regular (vaginal) sex, but that AIDS was really only a problem for gay men and
heterosexuals who injected drugs. Tell me, Dr. Pezzi, did the media lie to
us? Have they wrongly instilled a fear in us heterosexuals who don't use
drugs? Why did it take so long to expose this myth? Thank you for
your time, Jeff.
A: Yes, Bernard Goldberg is correct: the media lied about
this. Why did it take so long for the truth to come out? I've been
writing about this for years, and some doctors who are far better known than I
am have said the same thing. However, if the media disagrees with either
your message, its implications, or how it is presented, they will quash your
message. The media love things that are politically correct whether or not
they ARE correct. Regarding the notion that heterosexuals should be
shaking in their boots about AIDS, some people speculated that the media spread
this myth to curry favor with homosexuals, or perhaps because the media seem to
have taken it upon themselves to sanctify and champion the causes of anything
dealing with homosexuality, homelessness, minorities, and women's rights.
Homosexual men, of course, have good reason to fear AIDS. They also have
good reason to make us believe that we're all at risk for this disease.
Why? Because it makes it so much easier for them to get funding to support
AIDS research.
I know we like to think we live in a time in which such a propagandized
distortion of the truth doesn't occur, but unfortunately we often can't get our
facts straight even when they're not laden with deep sociological
implications. Take something as simple as body temperature. Ask
doctors what is normal, and 99% will answer, "98.6° F." You've
probably heard that a million times, too. There's just one problem:
this number is based on research done in the early 1800's, and was passed from
generation to generation with few people questioning its validity. The actual
average body temperature is about 97.6°. In the morning, it's about a
degree lower, and later in the day it's usually a degree (or more) higher,
depending upon activity level and other factors. I don't intend to turn
this into a treatise on body temperature; I just want to point out how we're so
susceptible to believing things if we hear them often enough.
In the case of the myth about how heterosexuals should fear AIDS even if they
don't abuse injectable drugs or engage in anal intercourse, there is more to how
this myth gained credence than mere repetition. During my years of
training, I'll never forget the subtle but unmistakable brainwashing I and my
colleagues were subjected to regarding this matter. I could spend hours
writing about that experience, but the bottom line is that we were pressurized
into adopting certain attitudes toward homosexuals and their — oops, OUR —
disease: AIDS. I don't favor ignoring AIDS research just because it
will likely be of tangible benefit only to gay men and drug-abusing
heterosexuals, because I think every taxpayer is justified in wanting more
federal dollars to fight "his" disease. Michael J. Fox wants
money for research on Parkinson's disease, Mary Tyler Moore wants more diabetes
research, and on and on. We all have our pet projects and interests, and
just because someone has a vested interest in funneling more dollars to something
that threatens him doesn't make that cause any less worthy. Hence, I don't
object to the fact that gay men want more money to research AIDS. Instead,
what galls me is the ease with which the truth of this matter has been
trampled. Unfortunately, this deliberate distortion of the truth has left
in its wake a lot of collateral damage. I've seen heterosexual patients in the ER
sobbing uncontrollably, worried that they may have contracted an HIV infection
just because they had vaginal intercourse. What used to be one of life's
greatest pleasures is now something that we often fear more than Russian
roulette. The needless hand-wringing engendered by this pervasive myth
about how HIV is spread has damaged many lives, causing people to fret about an
unfounded fear. We all have enough real fears to conquer without losing
sleep over things that aren't worth worrying about.
How much time do
you spend worrying about whether you will die in a car accident? Do you stop
driving and huddle under your bed just because many people die in car crashes?
No, because automobile transportation is too vital to life. Well, sexual
pleasure is one of the foremost things that makes life worth living. It is
prudent to be cautious, but don’t let fear rule your life.
I discussed this subject in more detail
elsewhere on my web
site. You may also wish to read The Myth of Heterosexual AIDS by Michael Fumento.
Yes, heterosexuals can contract an HIV infection, but if heterosexuals don't use
contaminated needles or engage in homosexuality, their risk of acquiring AIDS is
vanishingly small. In fact, one state that once required HIV testing
before issuing a marriage license ended that requirement when so few positives
appeared — remember, those people may not have acquired HIV via heterosexual
means, but rather by drug abuse or sporadic homosexuality.
Let's put this risk into perspective. I've seen several people killed
during traffic accidents while on dates. I've seen people who died while
engaging in sporting activities. I've seen men who died at work.
I've seen people who died from a faulty furnace. As a former ER doc, I've
seen people die in just about every way possible, yet I've never seen a
non-drug-using heterosexual die of AIDS. But do people worry about dying
in traffic accidents on dates? Or do they worry about dropping dead while
playing sports? Or at work? Or sleeping at home? No.
Virtually no one worries about such things, although those and dozens of other
seemingly innocuous events are far more likely to kill than vaginal
intercourse. Do you see how the media have twisted the facts?
Heterosexuals now think of sex as a potentially lethal event that is one of
their gravest threats. Does this make any sense to you? Virtually
every heterosexual who isn't an IV drug user dies of something besides AIDS, but
the media do not harp about this — they rant about HIV as if we had good
reason to make this our supreme fear.
The HIV virus has been so politicized that it will be years, if ever, before
people put this into proper perspective. As a doctor, I'm flummoxed by the
fact that people are usually oblivious to infectious agents and diseases that
are far more of a threat to them than is the HIV virus. I am not
encouraging people to take unnecessary risks with their health, but only to
spend more time worrying about their greatest threats and less time fretting
over less likely dangers (see the following question). Let's face it — no
one has enough time to worry about every risk we face, because everything we do
carries some risk. I could be killed while snowmobiling, because there are
plenty of kooks in that sport who drive at grossly excessive speeds on the
trails. Or I could be killed while mowing my lawn. It's hilly, and
riding lawn mowers occasionally tip over and crush their riders. Or I
could drown, be hit by lightning, or be crushed by a falling tree while logging.
After three close calls, I invented a way to cut down trees from a safe
distance. This is the correct way to deal with risk: identify
what is most likely to kill you, then think of a way to reduce that danger.
Incidentally, I also invented various ways to reduce the risk of STD
transmission, and I'll announce these in future editions of my book.
Relevant article: Celebrity promotion of charities 'is largely ineffective' says research
Dismantling a common myth about the transmission of STDs
(If you haven't already read the text in the
yellow box that preceded the above topic, please do so now.)
Q: You've answered
somewhat similar questions on your excellent web site, so I thought I'd write to
you for advice. My college prof assigned us to write a paper on a sexual
misconception. Anything come to mind?
A: Yes. I've received so many requests from college students asking
for help with their papers that I've begun to wonder if I should offer a service
writing term papers for a fee. :-)
There are countless sexual misconceptions, but since you're in college, I
presume your teacher is not interested in shattering myths that prevail only amongst
teenagers and the proletariat. To impress your professor, you need a myth
that even an intellectual might fall for. OK, here goes.
Nowadays, people usually interrogate prospective sexual partners before sleeping
together. The tacit message I've seen in innumerable sources is this:
your risk is decreased if your partner has had few sexual partners. This
seems so intuitively obvious that you may wonder why I am discussing it.
Why? Because it is misleading. Let's analyze this. This
simplistic assumption would be true if disease transmission were
100% per sexual experience, but it is not. For example, from one act of
intercourse, the risk of female-to-male transmission of herpes is 0.05%;
male-to-female spread occurs 0.2% of the time (you might hear somewhat different
statistics from various sources). While the odds are worse for gonorrhea
(female-to-male, 20%; male-to-female, 70%), gonorrhea is easily cured. The
risk of HIV transmission varies with type of intercourse (vaginal versus anal)
and presence of lesions, like herpes, that break down the vaginal lining or
penile skin. If those lesions are not present, some docs think that
vaginal intercourse is very unlikely to spread HIV. Some physicians and
scientists say the risk is zero, or close to it. I doubt the risk is zero,
because virtually everything carries some risk — even drinking water.
For
the record, I've had more patients die
from using a blow dryer than from AIDS if they were heterosexuals who
never used drugs or engaged in anal intercourse. I've also had more
patients succumb from welding, chainsaw or mower injuries, snowmobiling,
hunting, jogging, alcohol abuse, drug abuse, overeating, smoking, driving to
school or church, drowning, climbing in trees, or stupidity (like touching live electrical
wires while standing in a pool of water). A few years ago, Americans were
treated to a spate of brief public service commercials in which somber
Hollywood celebrities gave us condescending short speeches about AIDS. Ask yourself
this question: if prevention of death is the goal, why have I seen a
thousand commercials about AIDS and none about chainsaws, obesity, or the
hazards of electricity? Hmmm? I suppose those celebrities get
their information from biased sources that give them a skewed perspective.
I obtained my information firsthand. When a man was cooked by electricity,
flattened in a car accident, or died in any one of numerous other obvious ways,
I did not need a pathologist or medical examiner to tell me why he died.
Nor did I need some politically motivated statistician or spokesperson to tell
me what is killing 99.9% of Americans. I've seen tens of thousands of
patients, so my sample is large enough to be statistically valid. From
this, I know that heterosexuals spend their time worrying about the wrong
things. Instead of worrying about AIDS, it would be far more logical to
worry about dying from food that your spouse cooks for you. Remember
Poppin' FreshTM, the adorable little Pillsbury
DoughboyTM? Or Betty Crocker®,
Mrs. Butterworth’s®, and similar icons?
The processed foods they represent have contributed to the death of more
heterosexuals in the United States than has the HIV virus. This is
probably true even when heterosexuals are not excluded because of shooting drugs
or engaging in anal intercourse, and it is undoubtedly true when these risky
subgroups are omitted. Obesity, heart attacks, diabetes, strokes, cancer —
those are the big killers that people should worry about. Dr. Dean Edell
recently reported a study that suggested the high rate of heterosexual
transmission of AIDS in Africa is not due to sexual intercourse (as had long
been presumed) spreading a different subtype of HIV than is prevalent in the US,
but is instead due to unsafe medical practices such as using dirty needles.
Interesting.
The bottom line from the preceding discussion is that the risk of acquiring some
sexually transmitted disease from one episode of intercourse is less than 100%,
and very low for the incurable diseases that concern most people. Thus,
what matters more is not how many people you've slept with, but how many times
you've slept with them. I've been exceptionally careful about who I sleep
with, and my precoital interrogatory/investigation is probably more thorough
than that of just about anyone else. However, most people are not so
careful, and they gloss over subtle hints that would be red flags for me.
If they're horny, they jump into bed. Thus, the risk these people assume is
unknown to them. What difference does it make to switch from Partner #1
with an unknown risk to Partner #2 with an unknown risk?
I will illustrate this by looking at a hypothetical example. For the sake
of simplicity, assume the risk of spreading a disease is 1% per sexual
encounter. Assume that Person A had sex with eight partners, and Person B
had sex with four
partners. Who has a higher risk of acquiring the disease? That's
right, you cannot determine risk based on number of partners, so I will give you
more data. Person A slept with each partner twice, and Person B slept with each partner 20 times.
We should also know the prevalence of the disease. Let's say that is 1%.
Now who is more likely to acquire the disease? Let's do the math:
Person A
8 partners x 1% prevalence = 8% chance
of encountering a partner with the disease
8 partners x 2 sexual encounters per partner = 16 episodes of sex
16 episodes of sex x 1% chance of transmitting
the disease per encounter if the disease is present x 8% chance of
encountering a partner with the disease = .0128 = 1.28% chance of acquiring the
disease
Person B
4 partners x 1% prevalence = 4%
chance of encountering a partner with the disease
4 partners x 20 sexual encounters per partner = 80 episodes of sex
80 episodes of sex x 1% chance of transmitting
the disease per encounter if the disease is present x 4% chance of
encountering a partner with the disease = .032 = 3.2% chance of acquiring the
disease
Therefore, although Person B slept with half as many partners as Person A,
Person B is over twice as likely to have acquired the disease. Thus, the
most important factor isn't number of partners, it is the total number of sexual
encounters. If Hollywood folks are smart enough to lecture us about
staying safe, why don't they give us the real story? Don't they teach math
at Hollywood High?
A
very pretty virgin is falling for a man who had 350 partners
Q: Dear Dr. Pezzi:
I am a 30-year-old woman and will be having sex for the first time in a couple
of weeks. The reasons why I waited so long vary. I wanted to be in
love with my "first" and I haven't been in love since college (he was actually
sleeping with one of my friends while we were dating; I found out right before
the big event and broke up with him). I have also been very focused on my
career and let my personal life slide. The person that I am dating now is
someone that I have known for years. We have always had "feelings" for
each other, we have great intellectual chemistry, and our physical chemistry
(thus far) has been very good. We didn't date before this because he was
also very focused on his career and wanted to sleep around as much as possible
before we tried dating. He (and I) always felt that once we took that
step, that would be it, for both of us. He has slept around a lot (in the
hundreds), and although we have maintained a very close friendship over the past
couple of years I have not told him of my virginal status, nor does he suspect
that I am still a virgin. At the risk of sounding conceited, I am very
pretty, in great physical shape, and very well "put together." Men
constantly approach me (even a couple of his friends, who I frequently run into
at restaurants and at the gym). So he has no reason to suspect, nor am I
going to tell. This is the problem: as I mentioned he has had many
partners and I know he likes it "wild" (hair pulling, etc.) . . . and I suspect
I would as well. However, my conception of wild may be very different from
his, although I am not sure how. We recently saw a movie together (before
we started dating) that involved quite a bit of spanking. He asked me what
I thought about that and I told him that it looked like a lot of fun.
Honestly, I was thoroughly excited.
I want this to be great for him. I know it will be great for me no
matter what, because I am wildly attracted to him and very close to being in
love with him. I also know him well enough to know he feels the same way.
I have a couple of weeks to "prepare" (I am going out of town on business for
three weeks in a couple of days and we decided to wait until I came back).
Do you have any suggestions? Thank you, Clarissa
A: Yes I do, but before I delve into that, I want to address another
issue, namely "He has slept around a lot (in the hundreds) . . ." I assume you
mean that he has had hundreds of partners, correct? (Not one or two partners
hundreds of times.)
Q: Dear Kevin: Thank you for responding to my e-mail.
Regarding "I assume you mean that he has had hundreds of partners, correct?
(Not one or two partners hundreds of times.)": Both. He has had
hundreds of partners — probably around 350 over the past nine years, twelve of
whom he slept with hundreds of times ("friends"), maybe 150 "one nighters."
The remaining: sexual interaction occurred between 8 and 25 times
with each partner. For example, until recently he was sleeping with a
woman who lives in his apartment building. They weren't dating, they would
just get together twice a week and have sex (for the past three years), but he
was also dating and sleeping with other women (most of his dating relationships
would fizzle out around the 6th date).
Regarding the possibility of contracting an STD: he uses condoms, and
always has, except several times about 9 years ago (he was dating someone for
about two years, they were monogamous, and they didn't use them a couple of
times. He has always told me that he is very careful, always examines the
"area," and he never touches himself with the hand that has touched her.
He is also a surgeon and has a blood test every couple of months. However,
he has not been careful in respect to oral sex. He is quite comfortable
with performing cunnilingus, even on a complete stranger — which obviously
possesses (albeit a small) theoretical and demonstrated risk of STD
transmission.
At this point, I am more concerned with his inability/unwillingness to have
established or maintained an emotional relationship with any of these women.
He always said I was the standard by which he measured all women and they always
fell short. The more realistic explanation is, aside from
enjoying/appreciating the same things, we have incredible intellectual
chemistry. Most of his female companions are not intelligent. The
intelligent professional women that he dated are either un-cultured or
unattractive (by his standards). But still, 9 years of meaningless,
emotionless sex . . . is it possible he is addicted?
A: The short answer: yes. The long answer: You're
obviously an intelligent woman, so why can't you see that you're about to make a
major mistake? He has "DANGER" written all over him. Let's analyze
this in detail.
First, it is helpful to enumerate why people have sex. This may seem
overly simplistic, but I think this is the best way to make one of my points.
People have sex for procreation, to help cement a relationship, to give and
receive love, and simply for sexual gratification. Your prospective
partner (let's call him Bill) obviously is not having sex for the first three
reasons. You might think that his sexual appetite is fueled by the latter
urge, but I disagree. If sexual release was Bill's motivating factor, why
is he evidently perpetually on the prowl for someone new? Why isn't the
woman he had sex with last night good enough? Or the woman he slept with
last week? Or if finding a quality partner is so difficult for him, why
doesn't he just masturbate like the rest of us do? Why is he on a crusade
to boink enough women to fill a small town? Do women mean anything to him
other than giving him an opportunity to carve another notch in his bedpost?
Oh, I get it . . . Bill's quest for new flesh will end the day you sleep with
him. A switch will flip in his mind, and he will become monogamous.
A cozy home in the suburbs, a white picket fence, just you and him forever.
Does that strike you as plausible? It strikes me as wishful thinking and a
fanciful dismissal of the evidence. Ask a man to walk on the moon?
No problem. Ask him to change? Don't hold your breath.
You're probably thinking that things will be different with you and Bill because
you're hot enough to make him put down roots. Do you honestly believe that
Bill is so skilled at finding duds that he found hundreds of them who were such
losers that they deserved to be dumped once he had his jollies? Do you
think that Bill found 350 women who just wanted a fling? In my experience,
it is a rare woman who wants sex but not a relationship. Do you think that
Bill possesses some phenomenal ability to ferret out likeminded people? I
don't. I think that many, if not most, of his conquests believed that they
were special, too, and that they had a future with him. Marrying a
surgeon? Gee whiz, that is almost as desirable as bagging a rock star.
Bill is obviously attractive, charming, and successful . . . and you think that
he found countless women who just wanted an affair and nothing more? It is
a safe bet that this isn't true, and he knew it. Nevertheless, he was
slick enough to make them believe otherwise. He's undoubtedly suave and
skilled at making women presume that sleeping with him is a worthwhile
investment. You think so, too, don't you?
Some of the most charming and irresistible people in history were psychopaths.
Contrary to popular opinion, psychopaths are not twisted in every way at all
times. They don't reek of being aberrant 24/7/365. They can have
facets of utter normalcy, which gives them the ability to coexist with less
extreme people and not stick out like a sore thumb . . . except when they choose
to unfurl their tantalizing spells. After my training in psychiatry and
exposure to many thousands of patients in a variety of clinical situations, and
after I've pondered why people are spellbound by political leaders who are
clearly nuts, it is obvious to me that people are often magnetically drawn to
individuals who know how to exploit their unorthodox tendencies. They know
that many folks are just sheep who are eager to follow "the man with something
extra." The man who does everything by the book and abides by the rules
the rest of us follow — well, that man has "plain vanilla" stamped all over him.
We crave leaders who believe, and act, as if they are genuinely endowed with
singular powers.
I am not necessarily saying that Bill has psychopathic tendencies, but to bed
350 or so women requires a special "gift" that is worthy of an honorable mention
in The Guinness Book of Records. An average man has to work
overtime to sleep with ten partners, which is fairly typical. Yet your
Bill, in spite of the arduous years of medical school and residency, managed to
have sex with 35 times as many partners? Aren't you alarmed by such
off-the-scale behavior? Had he not been sidetracked by the nuisance of his
medical education, do you think that he would have stopped at a mere 350?
He is indisputably an avid believer in the notion that "more is better."
In fact, that seems to be his guiding light. Without that bothersome
diversion of med school and residency, he'd likely had given free rein to his
impulses and slept with enough women to erase your hope that his sexual appetite
is not incorrigible. Don't comfort yourself thinking that this is water
under the bridge. In the years to come after residency, he will have much
more time to pursue his personal interests. Don't believe me? Just
wait.
On to the next major obstacle standing between you and Bill and happiness
forever. If you read the topic about Why
does sexual pleasure vary so much from one woman to the next?
(presented earlier on this page), you know that the sexual pleasure men receive
from sleeping with women varies greatly — probably much more than the pleasure
variation women receive from different men, thus making it difficult for women
to comprehend this. After sleeping with hundreds of women, Bill is sure to
have found a few sexual superstars. If you aren't one, keeping Bill on his
leash is just a pipe dream.
Perhaps you think that sexual compatibility (e.g., the spanking you mentioned)
will suffice to keep Bill content. One might logically wonder how unusual
his sexual tastes are if he has yet to find a good match after 350 candidates
have not passed muster. Trust me, he's already slept with sexually
compatible women, and dumped them. Probably dozens of times.
On to the topic you knew I would discuss, so you preemptively attempted to
dismiss my concerns about it: disease. I will begin by stating the
obvious: Bill has not been too careful about choosing his partners, and
you don't need an MD degree to know that a quick visual check of the vulva is
not sufficient to exclude transmissible diseases. Next point: the
protection that condoms provide is far from absolute, and I've read convincing
statistical analyses by Ph.D.s who asseverated that partner selection is more
important than condom usage. Again, partner selection is Bill's Achilles'
heel.
By "blood test," I assume you mean testing for HIV and perhaps hepatitis.
But what about the other diseases? And what about your real danger, which
is that he's disease-free now, but may not be next Tuesday? I am not as
confident as you are that your intellectual and physical chemistry will reform
his ingrained behavior. He's had physical chemistry with others. And
surely in his storied past were at least a few women who were bright,
interesting, and vivacious. And what are they now? History.
I am alarmed by your statement about "Most of his female companions are not
intelligent." Does he purposely choose dingbats? Or is it so tough
to find 350 bed buddies that he is willing to scrape the bottom of the barrel?
Or does he somehow prefer to sleep with intellectually vacuous women, saving you
— The Prize, The Catch, The Complete Package — for long-term asexual
idolization? This is bizarre. If I were attracted to you and we
really hit it off (as you seem to have done with him), I'd want to sleep with
you, not a multitude of other women. If he were as fond about you as
you are for him, he would not have embarked on his jihad to sleep with every
willing woman. Some premarital sexual exploration is normal . . . but
three hundred and fifty? Does. Not. Compute.
I was also alarmed when you said, "The intelligent professional women that he
dated are either un-cultured or unattractive (by his standards)." When
99.9% of men meet women they find unattractive, they don't sleep with them.
Makes sense, doesn't it? What is it that compels Bill to buck this
commonsense tenet?
Back to the discourse on disease. The fact that he ends up twixt the
sheets with women who usually aren't brainy is something that heightens his STD risk.
Some things are too politically incorrect to be mentioned in the mainstream
press, so you may not be aware of the fact that the prevalence of STD's in dumb
people is much greater than it is in intelligent people. By definition,
dumb people do dumb things — one of which is to fail to exercise proper
precaution in the selection of sexual partners. Oh, the stories I could
tell you about this subject! I'll save those tantalizing true tales for
another book and just give you one of the lessons that I, as an experienced
doctor, learned in dealing with patients who saw me because they were concerned
after having sex with a new partner. The intelligent people, whose
circumspection made them wary, rarely acquired diseases. The dumbbells?
They'd be whimpering "Why did this happen to me?" as I explained the results of
their examination and tests and thought, "Because you slept with the wrong guy."
It's not that I am not sympathetic. I am. It's just that there is no
substitute for prudent avoidance.
All of which brings me back to you. You might not contract anything from
him initially, and he might remain forever faithful, although the chance of that
is slim. The one thing you cannot avoid is that having 350 partners is a
very bad sign. Please tell me that you are intelligent enough for this to
dissuade you from making a mistake that you may forever lament.
I've met docs like Bill before. One of them lost his medical license after
he had sex with a patient in the hospital chapel and videotaped it. Ripley
was right: truth is stranger than fiction. I am afraid that
years of "way beyond the norm" behavior have imbued Bill with the
idea that he can do just about anything. He might cool his jets for a
while, but when the 7-year itch hits (or for him, 7 months, if you're lucky),
he'll revert to his old habits. You might very well regret passing up
better, more stable opportunities by devoting yourself to him.
I'm sure you've heard that saying about, "Those who do not learn from history
are doomed to repeat it." Many of Bill's partners probably felt used by
him, and now regret sleeping with him. One of the advantages of reading
history and reading about others is that we can learn from their mistakes.
Wouldn't life be unbearably tough if we had to personally learn everything the
hard way? You have the luxury of having 350 women attest that Bill uses
women and discards them. And you want to be #351?
Sea-going husband suggests that his wife fornicate while he is gone; she fell
in love
Q: I am married to a
wonderful man who happens to be out at sea. While he was out he said I
could have a partner. I decided a threesome would be fun. So my
co-worker and her fiancé of five years decided to get together with me. It
has been three months now and things have been great until my friend's fiancé
told me that he thought he was in love with both she and I. And I felt the
same, but remember my husband who I also love is still out to sea. Now, my
husband knows about the threesome and when he gets home we are planning to
include him in the fun. I guess my question to you is this, can a person
be truly in love with two people at the same time? Or is there another
explanation for both his and my feelings towards each other and our spouses?
Thanks, Erica
A: Is there another explanation? Yes. You're lonely. And
him? Well, he is obviously not lonely.
Is he genuinely in love with you? I can't give you a definite answer based
on the limited information I have about your relationship, but there is a good
chance that he is confusing lust with love. Or perhaps you've both
succumbed to the pair-bonding effect of oxytocin (discussed earlier).
Is it possible to love two people simultaneously? Absolutely. We're
generally conditioned in our culture to confine ourselves to one romantic
partner at a time for pragmatic reasons, but consider this: is love
rational and based on definable reasons, or it is irrational and based on
nebulous and ethereal whims? People usually fall in love for identifiable
reasons: physical attraction, shared interests and beliefs, commonality of
intellect and sense of humor, complementary goals and personalities, mutual
admiration and respect, and yes, great sex. So if you love your husband
because he possesses certain attributes, why wouldn't you be very fond of
someone who was endowed with the same or substantially similar attributes?
The notion that "there is just one perfect mate for me" is sappy hogwash.
If love were predicated on this "one perfect match" nonsense, humans would have
gone extinct eons ago. Prior to the advent of motorized transportation,
people usually fell in love with others who were within walking distance.
Although we all have countless potential partners who would be good love
matches for us, we typically suppress those feelings — sometimes unconsciously and sometimes
with a great deal of conscious struggle. Loving more than one person at a
time is easy, but it is difficult for most people to accept that they are not
the sole love interest of their partners. To keep this from being a source
of friction, we usually nix the love for others . . . or try to act as if that
love never existed or was erased. Things are obviously different in your
little enclave. If your husband is so devoid of the usual male jealousy
that compels most men to throw a conniption fit when confronted with infidelity,
then he may also accept the fact that you love someone besides him. Given
that he is the one who suggested that some man pinch-hit for him in his absence,
he would be on shaky ground by proposing your
extramarital affair but bristling at the feelings of love that might foreseeably
result from it. That would be like suggesting that you strike a match, but
complaining that a flame resulted.
What
does sex feel like for the opposite sex?
Q: I'm curious as to what sex feels like for women. As a man, I know
just what sex feels like for me, but I doubt that it feels the same for women
because of differences in anatomy. I've asked my girlfriend to explain
what it's like for her, but she isn't telling me much by saying it feels really
good. As a doctor, I'm sure you have a much better understanding of the
differences in sensation between the sexes, and you can probably offer a much
better explanation. Thanks for solving this mystery, doc. Ben
A: Here is an excerpt from
The Science of Sex:
Sooner or later, most people wonder what people of the opposite sex experience during sexual stimulation. To understand this, you need to have at least a rudimentary comprehension of the development of genitalia before birth. Early in development, the sexes are anatomically indistinguishable. From this identical base, hormonal and other factors mold the genitalia into either the male or female form. The important point to grasp from this is that male structures have an analogous female counterpart in terms of origin, and vice versa. That is, the same tissue is sculpted into structurally different forms. While it may appear different, the
innervation — the way the nerves "hook up" — is essentially identical. From a purely mechanistic point of view in terms of sensation, the genitalia are nothing more than devices that stimulate the sexual nerves. Given that the nerves are identical, it is not surprising that the sensations experienced by the sexes are similar. Anatomical differences account for some minor disparity in sensation, but the overall experience is much the same. For example, when a man touches his scrotum, he feels what a woman experiences when she touches her labia majora (the hair-covered outer lips). Penile sensation is analogous to that of the clitoris, vagina, and labia minora (inner lips) combined. Just as a woman experiences different sensations when stimulation is alternated between the clitoris, vagina, and labia minora, a man will also experience different sensations when different areas of his penis are touched.
Having said this, it is important to note that there are differences in the sensations experienced by the sexes during intercourse. This disparity in sensation is attributable to two factors:
anatomic and tactile variation. The first results from the indirect stimulation of the glans clitoris during intercourse, as contrasted with the direct stimulation of the penis. The second factor, which is just as important, results from a variation in perceived sensation due to tactile (touch) dissimilarities between the penis and the vagina. Obviously, a penis does not feel the same as a vagina. Ergo, they cannot impart the same sensations during intercourse, even if the nerves supplying them are identical. For example, when a penis is touched by hand, and then by a vagina, the sensation is greatly different. Because the texture of a vagina differs from that of ordinary skin, the nerves are stimulated in a different manner. This difference in nerve stimulation results in a different nerve impulse, or signal, being conducted to the brain. The brain then interprets the variation in signals as variations in texture.
While the sensations during intercourse may differ, a very close appreciation of the sensations experienced by the opposite sex can be approximated when provision is made for the tactile variation of the penis and the vagina. Given the similarity in feel between the tongue and the lips (especially their inner lining, or mucosa) and that of the vagina, the sensations experienced by a woman when she is orally stimulated (cunnilingus) is quite similar to what a man experiences during intercourse, assuming that her labia minora and clitoral glans are stimulated. The sensations experienced by a woman during intercourse can be approximated in a man when he is orally stimulated by the moistened outer lips of the mouth on the dorsal (bottom) aspect of his penis, but there is no direct stimulation of the penile
glans.
Weight
gain after marriage and pregnancy: is it inevitable?
Q: I hate to admit this, but after my wife gave birth I am no longer
attracted to her. She had a good figure before pregnancy, but now she's
overweight. I've tried to get her to exercise or diet, but she won't even
try. Her doctor says her thyroid is fine, so that's not the problem.
I've noticed that many other women seem to permanently gain weight after
pregnancy. Is this something that is inevitable and men just need to
accept? Eric
A: It's not inevitable. The incidence of obesity in this country has
skyrocketed in the past few decades. Obesity is itself a disease as well
as being one of the primary contributing factors to heart disease, diabetes, cancer,
stroke, and arthritis. Therefore, obesity is not just a cosmetic
problem. Yet in spite of the fact that it is a serious and alarmingly
prevalent disease, it has become somewhat politically incorrect to think of this
as a problem. Instead, we're pressurized to accept obesity as being almost
inescapable. Men are made to feel guilty for desiring a svelte wife, and
we're told that we're putting unreasonable pressures on women by expecting them
to look like an actress, model, or Barbie doll. OK, it IS unreasonable to
expect every woman to be as thin as a stick, but is it really too much to ask
for today's women to have the same amount of body fat as women did a few
generations ago? In view of the fact that it used to be considered
unladylike for women to sweat, whereas exercise is now culturally acceptable,
you might think that today's women should be in even better shape. And
with the countless numbers of diet pills, diet supplements, fat-free foods,
weight loss books and clinics and whatnot, you might think that women should
be as thin as Barbie. Instead, we now have more women than ever who weigh
more than their husbands. The question is: why?
Before I answer that question, I should point out that I'm not gratuitously
slamming women. I used to be fat myself and I know how easy it is to gain
weight. However, I also know that anyone who wants to lose weight can
succeed. When I got out of my residency program I was so fat I couldn't
see my feet when I stood up. Now, even though I'm 14 years older, I have a
better body than most teenagers. I'm not mentioning this to brag; I'm
mentioning this to demonstrate that obesity is not some sort of inevitable
plague.
I will not address all of the explanations for obesity since many of them are
well-known and there are enough of them to fill a book. Instead, I'll
focus upon why women, more than men, are gaining weight.
First, let's discuss the "ripcord phenomenon." I don't know if
women discuss this amongst themselves, but every man I've known seems to know
about it — and fear it. In case you're not familiar with the
term, the ripcord phenomenon refers to the sudden ballooning of women after they
feel they've hooked a man . . . say, by getting a wedding ring or, for the
ultimate hook, by giving birth. Go ahead and scream about how politically
incorrect I am for discussing this, but remember that men were derisively
discussing this before I hit puberty and cared about what women looked
like. I'm the messenger, not the source of the message. The message
is that men like attractive women — surprise! — and that we're a bit
miffed when the women in our lives think so little of us that they give up
trying to be attractive. This stings all the more when men think that
woman don't try to lose weight because, thanks to the wedding ring or children,
they no longer need to even try. The hooks are sunk, so why lift a
finger?
Instead of pouting year after year about why men are so
commitment-phobic, magazines like Cosmopolitan could do their readers a
favor by forthrightly addressing some of the reasons why men are reluctant to
tie the knot — and one of these reasons is the fear of the ripcord phenomenon.
Or the editors of Cosmo might want to buy my $10 book (free if you buy my
sex book) in which I explain how it is possible to
lose
weight without dieting, drugs, herbs, exercise, or surgery. That might
seem as plausible as a perpetual motion machine or time travel, but it works and
the science behind it is basic physiology and physics. Not voodoo.
Not diets that only work for Hollywood celebrities. The problem is that
hucksters have promised us weight loss miracles for decades, and 99.99% of those
claims are either overhyped nonsense or a rehash of an old idea.
Consequently, it is natural that people are skeptical of weight loss claims —
especially ones that seem too good to be true. Alarmingly, the Federal
Trade Commission is trying to pressure the media into not accepting weight loss
ads that make "too good to be true" claims. The problem with stifling free
speech in this manner is that it presupposes that no miraculous breakthroughs
will ever occur — some of which may at first seem too good to be true. So
should physicians and scientists stop thinking and innovating, fearing that a
government bureaucrat with a room-temperature IQ could quash their ideas even if
they're legitimate breakthroughs? Haven't we been down this road before?
People who once suggested that the earth is round were lambasted by the folks
who "knew" the obvious, what they could see with their own eyes: the earth
was flat. And then there was the obviously premature idea circulating
around 1900 in which people suggested stopping research in physics, since
everything about physics was known. The atom bomb blew that supposition
apart.
Why do today's women seem to care less about their figures than women once
did? The answer is simple: because more women than ever work, they
don't need men. Collectively, enough women gained weight so that
the overall "mark" against which women are judged was lowered a notch
or two. After all, women use their looks (and other attributes, of course)
to compete for the best possible man. If enough women gain weight — and
this is just what happened — then what passes for an average woman is quite a
bit chubbier than before. If a man wants to get married, he often must
settle for a woman who is fatter than he'd prefer.
Interestingly, this ripcord phenomenon has not yet pervaded every part of the
United States, and certainly not every part of the world. Two summers ago
my friend Tracey and her husband, who live in southern Florida, came up to
Michigan, my home state. Tracey was flabbergasted and commented,
"What the hell is wrong with these women in Michigan? Almost all of
them are fat!"
One of the most common explanations for why there are so many obese women in
northern Michigan is that it's cold up here, so women bundle up. Since
layers of clothes can camouflage fat, the main theory is that this reduces the
incentive to diet and exercise. That isn't the sole explanation.
It's even colder in Minnesota, but the prevalence of obesity in that state is
much less. Go figure. Or consider women in Russia, many parts of
which are far colder than Minnesota. Women who place personals ads in
Russia typically describe their physiques as average when they weigh 100 to 110
pounds. In contrast, women in the United States (and especially regions
like northern Michigan) evidently think that 150 to 170 pounds is average.
That's even more frightening than what it may seem at first. Since the
weight of most non-fat tissue in the body (brain, blood vessels, liver, kidneys,
pancreas, bones, muscles, etc.) doesn't vary by much, a typical Russian woman
might have 20 pounds of fat while her "average" counterpart in the
United States may carry around 80 pounds of fat. What really matters isn't
body weight, it is body fat percentage. With rare exceptions, men think
that women with body fat percentages of 18% look yummy, while women who are 47%
fat by weight . . . well, not so yummy. Appearance aside, that extra 60
pounds of fat can cause a number of health problems.
Obesity is not inevitable. I beat it, and I know women who, even after
marriage and childbirth, have better bodies than most models.
I have other friends, too, like Karen, who are mothers yet have such stunning
bodies they'd make any man drool. Therefore, obesity after marriage or
childbirth is not certain. From reading your question, Eric, it seems
clear to me that your wife pulled the ripcord and doesn't feel the slightest bit
guilty about it. Is there a reason for this? Are you
obese? Is there a reason why your wife doesn't give a hoot?
Two years later I received this response from Eric's wife, Julie:
"Eric showed me your answer, and at first I wanted to strangle
you. You were right and I knew it, but rather than blame myself, it was so
much easier to blame you. However, deep down I knew that I had stopped
trying to keep myself attractive to Eric. Almost all of my friends are
overweight, and to tell you the truth that lowered the expectations I had for
myself. However, I guess I never really thought about how this might
affect Eric's feelings toward me. Anyway, I eventually faced up to the
facts. I was overweight, and I had a husband who didn't like my
body. I began dieting and exercising, and I regained my old figure.
You're correct, it can be done. Now our marriage is much better.
Eric treats me like he used to before we were married, and that of course just
fuels my desire to please him more. The passion had gone out of our
relationship, but now it's back. Thanks, Dr. Pezzi."
While it's politically incorrect and almost taboo to assail some of the
"games people play" in regard to obesity, I will discuss it because I don't
think that sweeping this problem under the rug is helping anyone. Obese people
often claim they do everything they can to lose weight even when they know
that's simply not true. Here's an example. I once met an overweight woman with a
number of good qualities. She was very interested in dating me, but I was frank
and explained that I am not attracted to obese women. She promised to lose
weight, so I continued to see her, thinking that we could develop a friendship
and perhaps more if she succeeded in losing weight. To make a long story short,
she put on a great show of trying to lose weight. Whenever I saw her eat,
she would either nibble at her food as if her stomach were the size of a
thimble, or she'd eat some atrocious homemade concoction like seaweed soup,
whose smell was reminiscent of feces. She told me that her workouts were
exhausting, but I didn't see any progress after this went on for months. Had she
ate as little, and exercised as much, as she claimed, after months of such an
arduous regimen she would have lost weight unless her body knew how to suspend
the laws of physics. I told her that I did not believe her, but she swore up and
down that she was doing everything she said. This protestation did nothing to
dispel my incredulity. No, really, she said. I'm trying, really trying, really,
really, really trying. Yeah, right. Sorry, I said, I still don't believe
you. Then she tried to persuade me using anger and a guilt trip. I didn't budge.
Finally, she sent me an e-mail in which she admitted that once she began seeing
me, she no longer felt an impetus to lose weight. Just what I'd suspected.
Between her periods of rigorously dieting, she'd binge enough to make up for the
earlier caloric deprivation. Finally, the truth.
Back in the days when I was fat, I could honestly say that I always starved
myself between meals. I pretended to be into health food. I could conjure up all
sorts of excuses as to why women should like me even though I was chubby. I
would focus on my good qualities, and ignore the reflection I saw in the mirror
after getting out of the shower. Self-deception and excuses became familiar.
Sound familiar?
As a resident working 110 hours per week, with no time to exercise, and with
food being the only pleasure in my life, I didn't even try to lose weight. I
suppose I could have continued this deception throughout my life and become one
of those physicians who use a doctor's smock to camouflage their dietary
indiscretions, but I'd had enough. I stopped the self-deception, and ended the
excuses. My metabolism didn't burn up calories as readily as it once did, but I
lost the weight. All of it.
Obese people often think that our culture picks on them. In some respects, it
does. However, our culture also bends over backwards to facilitate
self-deception in obese people. Insurance companies revised their criteria for
normal weights. Loose-fit jeans are the rage, not so much for reasons of style,
but because our physiques often need to be housed in extra fabric. Obese people
have their healthcare costs subsidized by thinner, healthier people who pay
equal premiums. Childhood obesity is skyrocketing, and more prevalent than ever.
The obesity thought-police ignores this, and instead just breathes a collective
sigh of relief that more kids aren't anorexic. Doctors are increasingly afraid
to address this problem, fearing that the parents will jump all over them for
mentioning anything that might interfere with their children's self-esteem. A
case in point. A ten-year-old girl had a potbelly due to the usual suspects:
too much food and not enough exercise. Not kwashiorkor. No other excuse I'd buy.
I explained to her mother that the pre-pubertal period was one of the times that
existing obesity predisposes people to a lifetime of fighting fat, so I urged
the mother to help her child lose weight now. She already weighed more than some
adult women, and she'd not yet reached the age when women tend to pack on the
pounds. The Mom's response? Anger. Predictably.
Unfortunately for patients, doctors in the United States now often think of the
people they serve as customers rather than patients. This
ideological shift has effectively put a muzzle on docs, making them reluctant to
address even glaringly obvious problems—such as a young girl with a potbelly—out
of fear that the customer might be irate enough to take their business
elsewhere. Doctors with better "patient satisfaction scores" pat themselves on
the back, and are sometimes rewarded with more money. However, by abnegating
their responsibility to do what is best for their patients, they're not doing
them any favors.
Is
it shallow for men to desire slim partners? Absolutely not. Here's
why.
An overweight friend of mine sent an e-mail to me in which she more or less said
that she's perfectly happy being overweight, and she suggested that men who
desire slim mates are shallow. My response to her presented a cogent
reason why it is not shallow to desire a slim partner. You can read
our e-mail exchange, or just read my central argument in the following
paragraph:
Marriage isn't just about today — it's about tomorrow, too. And a lot of tomorrows in the future. Obesity predisposes people to many diseases. Frankly, I don't want a wife who can't take a walk with me in the future because her knees or hips are arthritic. I don't want a wife who died years ago because of breast cancer. I don't want a wife who is tethered to an oxygen tank, and I don't want a wife whose body is destroyed by diabetes. I don't have a crystal ball to peer into the future and see who will be healthy, and who won't. So I judge the likelihood of poor health in the future by looking for the underlying factor
(obesity) that is the most frequent common denominator in the diseases most apt to kill or debilitate in the years to come. Therefore, being slim isn't just a matter of beauty; it's a strong indicator of long-term health. I don't have a crystal ball, but I do have common sense. Many other men have common sense, too, and their bias against blubber isn't some shallow desire.
Vaginal Contraceptive Film
Should masturbation be taught?
Today's "sexperts": they're sexy, but are they knowledgeable?
Q: What do you think
of vaginal contraceptive film? Susan
A: Not much. Coincidentally, I just saw a commercial for VCF®
Vaginal Contraceptive Film in which former Surgeon General Joycelyn Elders said
it's "the non-hormonal contraceptive you can't feel."
Really? I wondered if she's ever used it. Probably not.
There is nothing like hands-on experience, or in this case . . . well, I'm sure
you get my drift. I used it, back in the days when I had a girlfriend, and
found that the film dissolved into a gooey, tenacious mess that seemed stickier
than glue. Now for the bad news: it seemed to absorb the lubrication
naturally present in the vagina. Or perhaps it didn't truly absorb it, it
may have just felt that way because it was so sticky. I tried adding
lubrication, but within seconds I was back to sticky ol' square
one. Plus, like all contraceptives containing nonoxynol-9 as the
spermicide, it tends to cause a burning sensation. So, from an aesthetic
standpoint, I'm not very fond of it. Could you tell?
Its manufacturer touts that it has "an effective rate as high as 96% when
used properly." That sounds impressive, but keep in mind that the
real-world effectiveness of contraceptives is usually less than their maximum
effectiveness "when used properly." People who have sex are
sometimes too drunk or in too much of a hurry or are fumbling too much in a dark
room to properly use a contraceptive. Here's one of the flaws of VCF®
Vaginal Contraceptive Film: I think it takes too long to dissolve. I
have patience — anyone who can design and build a copying machine from scratch has
patience! — but that patience was sorely tested by waiting . . . and
waiting. From their instructions, I inferred that it dissolves in 15
minutes. Not in my experience. Another problem is that its
manufacturer states it should be inserted "not more than one hour
prior to intercourse." That led me to believe that its effectiveness
will decrease over time. So what do you do if intercourse is
prolonged? Insert one VCF® per
hour, then withdraw for at least 15 minutes before resuming intercourse?
However, this won't be a problem for you if you like VCF®
as much as I did, because you won't want intercourse to last more
than an hour — trust me!
OK, I'm through bashing VCF®
Vaginal Contraceptive Film. Now I'll take aim at the person who shilled
for them, the esteemed former Surgeon General. As you may recall, Dr. Elders was fired for advocating that masturbation be
taught. Such a radical idea offended the sensibilities of her boss,
President Bill Clinton, a man renowned for his morality. I'm certainly not
a prude, as should be evident from my forthright discussion of sex, but I think
that anyone who thinks masturbation needs to be taught has a few screws loose or
isn't running on all 8 cylinders. For heaven's sake, as a doctor I learned
that even simpletons were quite adept at pleasuring themselves. Come
to think of it, every male dog I've had seemed to be an expert in that! So
this is something that needs to be taught to humans of normal or even superior
intelligence? Why? I'll answer that quasi-rhetorical question by
opining that many of our "leaders" in Washington are people with
second-rate minds, and their dearth of brainpower sometimes leads them to latch
onto a questionable crusade, as in the Elders' initiative to teach masturbation,
as a way of justifying their professional existence. That may make them
feel good about themselves, but such a flimsy raison d'être would likely cause
the Founding Fathers to turn over in their graves.
In my mind, there is only one justification for teaching masturbation, and that
is when people are taught advanced techniques. People don't need an
introductory Masturbation 101 primer, but some could benefit from a postgraduate
Masturbation 899 course that goes way beyond the basics. Why?
If people were taught masturbation techniques that substantially replicated the
pleasure of intercourse, young people would be less inclined to engage in
premarital sex and thereby expose themselves to sexually transmitted diseases,
unintended pregnancy, and the burdens of that pregnancy. The compulsion
for intercourse is primarily fueled by one thing: the desire for pleasure.
People seem to have an innate realization that intercourse feels better than
masturbation, so humans — being the pleasure-seeking creatures that we are — do
what feels best. Thus, I think that parents, church leaders, and teachers
should not think that they've done everything possible to guide the next
generation simply by giving them the "thou shall not boink before marriage"
admonition. Behavioral psychologists know that people are more likely to
not engage in unwanted behavior if they're given an equally pleasurable
alternative, instead of just being told "no." Considering our abysmal
track record at curbing premarital sex, you might think that the need for a
fresh approach would be obvious. However, we're usually more interested in
conforming to the standards of hidebound propriety and doing what everyone else
is doing, rather than doing the right thing.
I've read a lot of material about sex and masturbation in college, medical
school, and the years thereafter in preparation for writing
The Science of Sex,
and I've yet to find an author discuss what I consider to be advanced techniques
of masturbation. Instead, sex authors are doing what they do in every
other area of sexuality, and that is just rehashing what countless others have
said. What an utter waste of time! If you read my book, you'll see
that I discuss groundbreaking subjects and give a fresh approach to old ones.
Rather than giving you exciting new facts by experts who are brimming with
knowledge, the latest trend is for sex authors to be gorgeous young women whose
claim to fame is based on appearance, not knowledge. This new breed of
sexologist is comprised of individuals without advanced degrees (or any
degree, in some cases) and without anything novel to say. Yet we
Americans, enamored as we are with appearance, put up with the drivel emanating
from these babes. So why is there a market for their echoing of ideas that
were old news a few decades ago? Because they look sexy.
Publishers know that readers often purchase books because their covers are
alluring, not because the content is noteworthy. Therefore, it isn't
surprising that these "sexperts" are often provocatively pictured on their book
covers. Taking this trend to an absurd extreme, one of today's hottest
sexperts is pictured throughout her book. No matter what page you turn to,
there she is, again and again. Isn't this an egregious waste of space?
If a book is worth reading, that space should be filled with worthwhile
information, not a picture that is repeated a hundred times.
Is
it selfish for a man to not want to use condoms?
Why women should dislike condoms as much as men
Q: My fiancée won't use any form of birth control other than condoms, and
she wants this to be our form of birth control even after we're married.
Needless to say, I'm not very happy about that. Is there a way for me to
discuss this so that I don't come off as being selfish? Do you think it is
selfish of me to NOT want to wear a condom? She says she cannot use the
Pill. Can you suggest other options? Ben
A: First of all, I do not think it is selfish of you to object to wearing
condoms. Sexual pleasure is the most intense pleasure that people can
experience, and condoms substantially reduce this pleasure for men.
Therefore, by insisting that you wear condoms, she is blithely asking you (or
telling you) to forgo that supreme pleasure.
I don't think that it is in her interests to cavalierly disregard your
pleasure. Sexual pleasure is the primary glue that binds men and women
together. If you think I'm overstating this, consider the likelihood of
marriage or other lifelong commitment if you could not have sex with your
partner. In that case, why bother? You could assuage your need to
talk to women by maintaining close friendships with them, couldn't you? I
don't know any man who'd be willing to accept the responsibilities of a marriage
without sex. She isn't asking you to abstain from sex, but she is
evidently willing to toss down the drain a lot of the pleasure that you deserve
as a husband. That isn't good for her, either, because when sexual
pleasure is diminished, so is the strength of the bond between a man and a
woman. That is one reason why I think it is important to amplify sexual
pleasure as much as possible, because when it is enhanced, so is the strength of
the bond between the couple. Furthermore, sexual activity fosters health
in many ways. However, it is important to realize that the quality of the
sexual experience varies from disappointing to heaven on Earth, and the health
benefits are commensurate with the pleasure: so-so sex isn't as conducive
to health as is fantastic sex. Therefore, in
The Science of Sex I discussed many ways to intensify
sexual pleasure.
If your wife cannot truly use the Pill, then there are many other
alternatives. Perhaps the best one for long-term use is an IUD. When
women hear IUD, their knee-jerk reaction is often, "An IUD in my
body? No way!" IUDs acquired a bad reputation because the ones
used years ago often caused problems, but the modern IUDs are one of the safest
and most effective birth control options available. If I were a woman, my
first choice for birth control would be an IUD. I don't know your age and
whether you plan to have children, so other birth control options such as
vasectomy or tubal ligation should be considered. If you and your fiancée
can tolerate the burning induced by most spermicidal contraceptives and you
aren't troubled by their lower rate of effectiveness and aesthetic drawbacks,
then those might be viable alternatives.
Women often incorrectly conclude that they "cannot use the
Pill" because they fear one of its potential side effects without
considering some of the positive aspects of using oral contraceptives. For
example, while the Pill may increase the risk of breast cancer, it reduces the
risk of ovarian and endometrial (uterine) cancer and may reduce the risk of
colon cancer, too. As a general rule, it is shortsighted to consider only
the negative aspects of using a drug without also considering its benefits,
too. This one-sided viewpoint often leads some postmenopausal women to
conclude that they'd be better off without supplemental estrogen. In
reality, estrogen therapy has many more benefits than risks. Even if women
ignore their quality of life and appearance (which are substantially better with
estrogen), the overall risk of death is less in women who take estrogen than in
women who do not. (I discuss this subject in my book because the media
have twisted the facts in regard to postmenopausal hormone replacement therapy.
"The media" largely consist of people with degrees in journalism, not medicine.
It shows.)
Hedonistic
calculus and the Pill: are women who insist on condoms selfish?
Q: My wife refuses to use the Pill, saying that no man ever died of a
blood clot caused by a condom. I HATE using condoms, but when she presents
her argument against the Pill this way, my reluctance to use condoms might seem
selfish -- as if I care more about my pleasure than the health of my wife.
Your thoughts?
A: Look at it this way. If she insists on condoms, there is a 100%
chance that such usage will decrease your pleasure. On the other hand, if
she used the Pill, there is an excellent chance she'd never develop a blood
clot. Thus, she evidently believes that the remote risk of a blood clot is
more important than the certainty that using a condom will substantially
diminish your pleasure. Now who is being selfish?
I've yet to see a woman with a blood clot caused by the Pill. Yes, I've
read the studies, and I know that the risk of thromboembolic events is increased
when women use the Pill. But if this were a common occurrence, after
treating many thousands of women, I would have had at least one who developed a
blood clot while on the Pill. Interestingly, I've treated several women
for blood clots, none of whom were on the Pill. This brings up an
important point. If those women were on the Pill, everyone would
reflexively blame the Pill for the clot. However, women develop clots for
other reasons (smoking, bad veins, bad genes, a diathesis to clot, random
chance, angry Gods, etc.). Hence, many clots that are blamed on the Pill
would have occurred even without it, but because some women on the Pill develop
blood clots, the Pill is blamed for the clot — often incorrectly.
Given the variety of alternatives, I don't know why people sometimes think that
the choice of a contraceptive is either the Pill or a condom. In any case,
if you cannot change your wife's opinion, you should consider using a subcondom,
as I discuss in my
book. This can increase pleasure for both partners, for reasons
I explain therein. While using a condom with a subcondom is more
pleasurable than using just a condom, it isn't as pleasurable as intercourse
without a condom. Since sexual pleasure is not something that should be
cavalierly disregarded, I think women should consider this when making a
contraceptive choice.
Hedonistic calculus is Bentham's strategy for balancing the pleasure or pain
that a given action is likely to generate, and hence whether that act is
desirable or not. While hedonistic calculus sounds like something that'd
interest only pointy-headed academics or students of philosophy, we all
intuitively use such calculus in making decisions in our lives. I enjoy
riding motorcycles, but consciously choose not to do that any more because of
the risk of that activity — which is why ER personnel sometimes refer to
motorcycle riders as "organ donors." Whenever I hear wives
insist on condom usage, as if their health meant everything and their husband's
pleasure meant nothing, I always think of how hedonistic calculus applies to
other facets of marriage. For example, in my years of working in the ER, I
had ONE woman who died on her way to work and NONE who died at work. In
contrast, I had countless male patients who died either commuting to and from
work, or while at work. Generally, men assume the riskier occupations and
often commute longer distances. I think it is second nature for men to refuse to allow women
to perform genuinely dangerous work. While this can be analyzed ad infinitum
by a variety of perspectives (Darwinian, pragmatic, social, etc.), the bottom
line is that men are willing to assume some risk in order to benefit their
partners. No doubt, many women do this too. However, some women —
and your wife appears to be one of them — fail to appreciate that a good
marriage involves broadening their perspective of hedonistic calculus to include
not just what is best for them, but also what is best for their partners.
I'll now dispense with the highfaluting discussion of hedonistic calculus and
present this matter in shirtsleeve English. When I hear female sexologists and
other professionals clamoring for condoms, I think, "That's easy for you
to say." Their enthusiasm would no doubt be tempered if condoms deadened their
enjoyment. In my mind, they would be far more effective if they acknowledged the
disparity of pleasure reduction between men and women, and discussed ways to
reduce it (such as by using subcondoms, or forgoing condom usage and making
better decisions about whether a given partner is an acceptable risk or not).
The usual chatter about this is too simplistic and narrow in scope. As an ER
doctor, I learned that sexually acquired diseases are far more common in certain
groups — and I am not just referring to the well-known ethnic and racial
disparities, either. The prevalence of sexually transmitted diseases varies with
occupation, intelligence, personality type, locale, and other factors. People
who know what to look out for can usually boink to their heart's content and
stay safe. On the other hand, people who are clueless often acquire an STD the
first time they hop into bed with someone. Very predictable.
Why
vaginal laxity is a problem that most men simply cannot discuss with their wives
Q: For the past few years my husband refuses to sleep with me. Every
night it is the same old story: he falls asleep watching television and
spends the night on the couch. This began shortly after I gave
birth. We resumed intercourse after my vagina healed sufficiently, but
that lasted only for a month or so. I don't know what the problem
is. Otherwise, I have a great relationship with my husband. He
doesn't use drugs or alcohol, and I know he's not cheating on me because he
works out of our house so I always know where he is. He still has a sex
drive because I sometimes see him masturbating when I walk into the bathroom
when he's in the shower. I don't have any big stretch marks, I lost all of
the weight I gained during pregnancy, and I work out regularly to keep myself in
shape so that can't explain why he's evidently repulsed by me. One of my
friends thought he may have the Madonna/Whore Syndrome, but I really don't think
so. We saw a counselor several times at my insistence, but my husband
never revealed just what is going on in his head to explain why our sex life is
a big zero. I've read all the usual explanations for why men lose interest
in sex after childbirth (such as wives ignoring their husbands), but none of
them seem to apply to our situation. He still says he loves me, but it
obviously seems more like the love of a brother for a sister. Do you have
any insight as to why he's acting the way he is? Pamela
A: Let me summarize this to put it into perspective: you have a
husband with an apparently intact libido who isn't having an affair, doesn't
otherwise manifest disaffection from you, and he "tried out" sex for a
month before giving it up? This is not one of the Great Mysteries of the
Universe. The most likely explanation is that he found
sex after childbirth much less pleasurable than it once was. This commonly
results from vaginal stretching and tearing during delivery. This affects
some women far more than others. A few lucky women seem to emerge
unscathed by vaginal delivery, but most experience some permanent dilation of
the vagina that reduces sexual pleasure for both partners, but men seem to be
more finicky and sensitive to this change than women. It isn't that
uncommon for a woman's vagina to be so stretched by childbirth that men find it
very difficult to obtain a gratifying level of pleasure from intercourse.
I've heard some men complain to me that they sometimes have difficulty telling
whether or not they're still inside the vagina because it is so loose. May
I let you in on a little secret, ladies? Judging by how often I've heard
men discussing this problem, men seem to have no difficulty discussing it with
other men. However, this is something than most men find almost impossible
to discuss with their wives. Even if you can appreciate how uncomfortable
a typical man is if he even thinks about bringing up his dissatisfaction
with his wife's weight, you probably have no idea how utterly impossible it is
for most men to discuss such a sensitive and potentially hurtful issue as
dissatisfaction over vaginal tightness. Many people are uncomfortable
discussing any sexual problems with their partners, and men may be
hesitant to discuss vaginal tightness because it may make them seem
shallow. However, I don't think that it is shallow for anyone to not want
to be shortchanged on life's greatest pleasure. Therefore, it is
unreasonable to blame men who are dissatisfied by this problem. Sweeping
this problem under the rug won't solve it, so what will? Men often aren't
great communicators, and it is sometimes easier for a man to keep silent, stew
over his disappointment, and chase after another woman instead of having the
courage to discuss this problem with his current partner. Ironically, men
who truly love their partners may not want to discuss topics that they feel
might emotionally wound their loved one. Hence, the problem is swept under
the rug, not solved, and the marriage slowly dissolves or remains perpetually
dissatisfying.
His choice to sleep on the couch likely results from the fact that he doesn't
want to take the risk that you might initiate intercourse. For him to
break off your advances would require some direct refusal that he might find
uncomfortable, whereas if he sleeps on the couch that is a very passive and easy
way to say no.
My advice for you is to see your gynecologist and ask him for his opinion on
whether or not your vagina is too loose. Don't assume that your doctor
would have already mentioned this even if he'd noticed it, because doctors are
usually trained to not point out a problem unless it may be serious. For
example, if a doctor noticed that a man had skin cancer and did not mention it
to the patient, that would be a serious mistake. In contrast, if a doctor
noticed that a man had an unusually small penis, the doctor certainly would not
comment upon this unless the patient first broached the subject.
Similarly, a doctor would be remiss for telling a woman that she had a loose
vagina unless she specifically inquired about that. I've performed pelvic
exams on many women who had loose vaginas (some of whom had never given birth),
but I never told them how tight they were unless they first asked me. A
woman with a loose vagina may have a husband with a large penis, so her vagina
may be just the right size for him.
If you want an immediate improvement in subjective tightness during intercourse,
you can use a vaginal wedge, as I discuss in
my
book.
Some people think that Kegel's exercises can completely correct
childbirth-induced vaginal loosening. In some cases, that is true.
However, in most cases — Kegel's or no Kegel's — there is a noticeable
laxity of the vagina after delivery. Surgery may be the only way to undo
the damage. I understand that some women feel an emotional compulsion to
give birth vaginally, but vaginal childbirth can cause problems other than
vaginal loosening. The following excerpt from Fascinating
Health Secrets discusses some of these problems:
Want to maximize the intelligence of your child? Deliver by C-section rather than vaginally. For a variety of reasons, some children born through vaginal delivery have compromised oxygen delivery for variable periods of time. This can be enough to cause some degree of mental deterioration. Only rarely is this pronounced enough to warrant a label or diagnosis such as "cerebral palsy" or "mental
retardation." If the child was otherwise destined to have a superior I.Q. and sustained some degree of hypoxia (low oxygen) during delivery, this might only reduce his I.Q. from 140 to 100. Since 100 is by definition
normal or average, it is difficult to retrospectively appreciate the tragedy which occurred during the birth of this child.
Since many C-sections are done only after some problem has already developed, a simple statistical analysis of the intelligence of children born via C-section versus vaginal delivery does not serve to adequately illuminate the cerebral risk of vaginal birth.
Unquestionably, if I were a woman, I would choose to deliver all of my children via C-section. Vaginal childbirth can be excruciating, and C-sections can be done almost painlessly. Furthermore, vaginal childbirth often permanently stretches the vagina and surrounding structures. This can reduce pleasure during intercourse for both the woman and the man. The stretching can also predispose a woman to prolapse of her uterus and other problems, such as stress incontinence. Stress incontinence, in case you are curious, has nothing to do with psychological stress. Rather, it refers to a momentary loss of urinary continence that results when the pressure within the abdomen increases as a result of coughing, sneezing, laughing, heavy lifting, or even something as seemingly innocuous as standing up. It may also cause a woman to discharge spurts of urine during sexual orgasm, which is often erroneously interpreted as representing a female ejaculation. While I certainly sympathize with women who are afflicted with this condition, who no doubt derive some degree of comfort by viewing their emission as an ejaculate, I am compelled to report that scientific studies on this matter have shown that such ejaculations are, in fact, nothing more than spurts of urine that are discharged from the urethra. While this problem can be minimized by the use of Kegel's exercises, the best treatment is obviously prevention.
The preceding topic prompted a
woman to write to me. The gist of her e-mail was this: "Well,
I've already had kids by vaginal delivery. My vagina is loose, I have
stretch marks, I've gained weight, my husband seems distant, and the sky is
falling. So, your advice may help women if they haven't yet had kids, so
they can choose to have a C-section, but what about us other women?"
My response? Generally, I eschew writing about topics unless I can offer a
solution. After all, what is the point of broaching a topic unless I can
suggest a remedy? I don't think it does much good to commiserate, so
you'll rarely find me wailing about an insolvable problem. Hence, when I
write about a problem, it's because I have the answer. And in this case, I
do. In my book, I discuss several ways to either tighten or effectively
tighten the vagina, such as by using a vaginal wedge. In regard to her
other laments, I presented solutions to them elsewhere in my books and web site.
A
too-tight vagina?
Q: I've been with my
husband for two years and we have had a sporadic sexual history. The frequency of intercourse declined from every day to once every
two to three months. I asked him why the change occurred and he gave me
several reasons, such as a poor adjustment to us living together, change in his
work schedule, and decrease in energy due to allergies. This year we got
married and began trying to have a baby. Our sex life improved slightly and we
began having sex once every month around my ovulation time. Recently I told my
husband that I would like for us to have sex more than once a month and he
finally told me that the REAL reason we don't have sex more often is because my
vagina is too tight and it causes him pain. It is worth noting that my husband
is the first uncircumcised man that I have ever been with and it usually takes a
second for my body to adjust to the width of his penis. But after that period of
adjustment is over, I truly enjoy having sex with him. Moreover, I always have an
orgasm. Can you suggest something that I can do to loosen up? Oh, we already
tried K-Y jelly and he says that it's still too tight. (Name withheld by
request)
A: I'm not going to beat around the bush: I don't believe your
husband. First, he offered some lame excuses, then he fessed up to the
"REAL" reason, your tight vagina. I don't doubt that your vagina is tight,
but tight enough to cause pain for him? Unless he has some penile
abnormality or has taken Accutane*, it is safe to say that he still isn't telling
you the truth. Why can I say this with confidence? Because sex is
pleasurable for you. Even though it usually takes a second for your body
"to adjust to the width of his penis" (which is common), you experience
pleasure, not pain. In my experience as a doctor, I've seen women with
vaginas so small that they'd tightly grip a pencil, and men who are hung like
horses and make male porno stars look like boys with pre-pubescent penises.
Even when the fit is tight enough so the woman is literally ripped open and
wincing with enough pain to cause her to go to an emergency room, I've yet to
hear a man complain about a painfully tight vagina. Instead, they're
dreamily marveling at how great a tight vagina feels.
* Some men who've used Accutane reported to me
that it made intercourse unpleasant and even painful, even after discontinuing
that drug. One man was so distraught over this that he was suicidal.
Incidentally, I've heard from several women who reported that Accutane made
intercourse painful, too. For more information on the adverse sexual
effects of Accutane, visit this web page.
When I was in medical school, my girlfriend had a vagina so tight that it took
me months of trying before I penetrated her — and that success was only due to
hours of patiently using a series of progressively larger dilators. By the
way, when I finally got in, it was pure pleasure, not pain. It sounds as
if your vagina isn't quite that tight in relation to the penile size, so it
doesn't make any sense that tightness is what is dissuading your husband.
Furthermore, even if tightness were the problem, your husband could
gratify you and himself by stroking his penis on your labia minora, clitoris,
and vestibule (the area around the vaginal opening). Or you could perform
oral sex on one another, or do other satisfying things.
I think it is apropos to briefly mention two scientific facts before I
proceed. First, there is a tidbit from physics, Newton's third law, which
states that for every action, there is an equal and opposite reaction.
This law is applicable everywhere, including the vagina. Translating this
principle of physics into everyday sexual language boils down to one simple
fact: the pressure or "tightness" is the same for the penis and the
vagina.
Next tidbit, this one from anatomy and physiology. When a woman
experiences pain from an overly thick (relative to her vaginal diameter) penis,
that pain is due to stimulation of stretch receptors. During
intercourse, a man's penis is compressed, not stretched. The
threshold for pain in stretching the vagina is far less than the threshold of
pain for compressing the penis. If the penis were stretched, it'd be
just as sensitive as the vagina, or even more so. Any man who doubts this
can prove it to himself by placing his penis in a vacuum/pressure chamber.
Noting the sensation when the absolute value (such as 5 psi, or pounds per
square inch) of the vacuum is the same as the absolute value of an applied
pressure, it is obvious than men will flinch with pain at vacuum levels
that are not unpleasant if that same number of psi is applied as a pressure.
However, because the penis is compressed, not stretched, during intercourse, the
penis is impervious to coital stretch pain. Practically speaking, the
threshold for penile pain in compression is so great that it virtually never occurs
during vaginal intercourse, except if the penis is very forcefully bent during
rapid thrusting when there is a mismatch between the axes of the penis and
vagina; that can stimulate stretch receptors. In general, any body part —
vagina, penis, arm, etc. — is more sensitive to pain from stretching than
compression.
Let's consider the foregoing two principles together. Because of Newton's
third law, I know that the pressure stretching your vagina during intercourse is
the same as the pressure compressing his penis. Because people are more
sensitive to pain from stretching tissue than compressing it, you would
experience pain from stretch long before he'd experience pain from compression.
The fact that you don't have pain indicates that tightness isn't the problem.
So what is the problem? I have my own suspicions, but I am not a
psychologist or psychiatrist, so I consulted several people who have expertise
in understanding problems in relationships. Incidentally, the initial
reaction of every person was the same; they thought it was preposterous that
your vagina was the source of the problem. They suggested a few
possibilities, such as him having a low libido, or inadequate attraction to you
(or perhaps to women in general). I may not be a relationship expert, but
in this case the answer seems so obvious to me that I'm willing to go out on a
limb and speculate about what I think the problem is. I think your husband
either now has the libido of an 88-year-old man, or his attraction to women is
questionable. In short, I don't think the problem is you. There are
many things that attract men to women. Some of these factors are optical
(that is, what a woman looks like), some are behavioral, and some are purely
sensual. Women feel good to men because it is pleasurable to hold you,
caress you, and make love to you. In regard to the latter point, your
tight vagina would make you very desirable, not someone to be sexually shunned.
You mentioned that you're now "having sex once every month around my ovulation
time." Unless that timing is intentional (to optimize your chances of
conception), this makes me wonder if the problem is your husband's libido.
Why do I think that? Because women emit more copulins (pheromones that
increases male libido) at ovulation than at other times. If a man
typically has a low libido, the boost in sex drive is more noticeable than if
he's always hot to trot.
As a next step, I'd ask your husband if he masturbates. If he does not,
and his sole source of sexual release is your monthly tryst, his libido is
clearly deficient. When men have a problem with their libido, they're apt
to conjure up a specious excuse, such as your husband attributing his lack of
desire to a "change in his work schedule." Stress of any sort can reduce
libido, but a mere schedule change won't decimate libido to the point that he'd
go from daily intercourse to once per month. When I worked in the ER, my
schedule would sometimes change five times in a week from the day shift to the
afternoon shift to the night shift. Sometimes I'd work two shifts in a
day, getting off from the night shift at 7 AM, going home to sleep for a few
hours, and then returning to work for the afternoon shift at 1 or 2 PM.
It's difficult to imagine a more chaotic schedule than that. In spite of
that nightmarish routine, my libido was reasonably intact and even brimming if I
had a girlfriend. Frankly, I've seen people hospitalized with serious
diseases or injuries who want sex more than once per month. Hence, I don't
buy your husband's stress excuse.
Your husband needs to see a doctor to exclude a penile abnormality (unlikely but
possible) or treatable causes of low libido, such as some pituitary tumors and a
number of other endocrine problems (some of which I discuss in my book,
The Science of Sex).
Now for the last plausible possibility: latent homosexuality. This
isn't rare, and it is often so well camouflaged that it may never have occurred
to you. A few of my friends and relatives were engaged to people they
thought were heterosexual, and when I met them, I didn't detect any clues that
might suggest otherwise. In all of these cases, they engaged in sex and
truly enjoyed it — from what I heard, which was sometimes through a very thin
wall. So, when their true sexual preference was revealed, I was stunned.
I wondered, how could anyone present such a convincing acting job? Our
culture is not very accepting of homosexuality, so this undoubtedly makes some
homosexuals reluctant to reveal their gender preference. However, I
wouldn't fret over this possibility. Statistically, the most likely
problem is a flagging libido. The good news for you is that this is easily
treatable.
What
really turns women on? A student doesn't want opinions, he wants proof.
He got it.
Q: I'm writing a paper for my creative writing class in college in which
I'm attempting to explain what male attributes are especially attractive to
women. Of course, women want men who are kind, attentive, and
considerate. But what about other attributes? What attracts women
more: brains, appearance, money, fame, or power? I have my own opinion
about that, but I don't know how to prove it. Obviously, I'll
receive a better grade on my paper if I can offer conclusive evidence to
substantiate my opinion. Can you help me? Thanks, Andy.
My answer to this question strays somewhat off the
topic of this forum, so I presented it on a separate
page.
Can
some sexual lubricants kill HIV?
Q: I just heard about a study which showed that some sexual lubricants can
kill the HIV virus. Is this true? Amanda
A: You're probably referring to a study led by Samuel Baron, M.D. at the
University of Texas Medical Branch at Galveston. He found that three
sexual lubricants (Astroglide, Vagisil, and ViAmor) reduced the rate of HIV
replication by more than 99.9% when those lubricants were mixed with
HIV-infected semen. However, those experiments were conducted in test
tubes, not humans. What works in vitro (in a test tube) doesn't
always work in vivo (in living beings). Furthermore, those samples
were allowed to sit for 24 hours because Dr. Baron said it takes some time to
deactivate HIV. I hate to be flip, but HIV would probably be deactivated
after sitting for 24 hours in a McDonald's malt, a glass of orange juice, or a
zillion other fluids that have no special anti-HIV effect.
Whether or not those lubricants prove to kill the HIV virus during sex, it is
nevertheless advisable to use a sexual lubricant if vaginal lubrication is
insufficient because adequate lubrication minimizes the risk of transmission of
various sexually transmitted diseases. If you're looking for a sexual
lubricant that kills HIV and potentially other STDs, I discuss a much better
alternative in my book.
Who
is the father?
Q: I have a question that's been troubling me for
a little over 2 years. I'm the mother of 2 beautiful girls and I don't know who
is the father of my second daughter.
This is the situation ... I had sex on and off with my first husband for 7
months when I lived in California. My last monthly period was on Oct. 30, 1998
and ended on Nov. 5, 1998 (regular menstruation). I had sex on Nov. 11, 1998 and
after that I left California and returned to New Jersey. I did not get my period
in the beginning of December. I had sex again with an ex-boyfriend on Dec. 23,
1998. After that I did not have any further sexual contact with either man. On
January 16, 1999 I found out I was pregnant. What confuses me is this ... On my
sonogram taken on February 3, 1999, it states that my LMP (last menstrual
period) agrees with my gestation period — it states I am about 8.6 weeks.
My question is if you could please help me in this matter ... and at least try
to give me a clear understanding of who could be the father of my second
daughter. This would take a huge load off my conscience. I would greatly
appreciate your help in this matter. THANKS A MILLION!
A: Based upon the timing of your intercourse, the most likely father is your first husband. However, when you state that your LMP "agrees with my gestation period...it states I am about 8.6 weeks," that doesn't mesh because if your first husband impregnated you, then you would have been about 13.7 weeks along. As a rule, pregnancies are dated from the first day of the last normal menstrual period. Therefore, it is possible that you skipped a period and the ex-boyfriend impregnated you. In that case, you'd likely be about 6½ weeks along on February 3.
It'd be helpful to know the duration of your cycles (e.g., are they 28 days?), their regularity, and so forth. What would be even more helpful to know is the blood type of the two possible fathers, your blood type, and your daughter's blood type. With that information, it may be possible to exclude one of the men as a possible father. That would save you the expense of testing for a DNA match
— which, of course, might cause the candidates for fatherhood to raise their eyebrows.
Pro
baseball player scoring on the road?
Q: My husband is a Major League baseball player who takes Viagra (no, he's
not the guy in the ads). My husband takes Viagra with him on road
trips. I confronted him about this, thinking that he cheats on me while he
is on the road. He responded that he needs the Viagra so he can
masturbate. Does this make sense to you?
A: Have you ever read Ball Four by Jim Bouton, the former major
league pitcher? In that exposé, he revealed the sexual escapades of
ballplayers, among other topics. I'm not suggesting that your husband is
necessarily cheating on you (he may suffer from the common misconception that
men need an erection to experience sexual pleasure and orgasm, or he may simply
find it easier to masturbate with an erection and he is willing to incur the
potential side effects of Viagra for this minor convenience), but I can
certainly understand why you are suspicious, given the track record of
professional athletes in regard to marital fidelity. I suggest you educate
your husband on this matter, teaching him that an erection is not a prerequisite
for masturbation to orgasm, and showing him ways (if he doesn't already know
them) to masturbate without a full erection. Afterwards, if he still
insists on using Viagra during road trips, he's either really stupid or he's
really stupid. Take your pick.
Disappointed
by wedding night
Q: I don't know how to put this. I'm stunned, disappointed, in
disbelief. I had sex for the first time last night on my wedding night,
and while it was pleasurable, it was not nearly as pleasurable as I assumed it
would be. Considering how much attention is paid to sex, I thought it
would be fantastic. It wasn't. Why?
A: Dang, where did I put my crystal ball, anyway? You didn't say if
you are a man or woman, so I can't address some of the most common reasons for a
reduction in pleasure pertaining to specific sexes. Instead, I'll discuss
this topic in a general sense. First, people are often disappointed by
their initial episode of sex. I was, too. However, in time,
intercourse became more pleasurable with that partner, and with a subsequent
partner, sex was so pleasurable it was beyond my wildest dreams — I had no
idea that such intense pleasure was possible. That was quite a change from
the "this is it?" shock and disappointment I felt after my
first time. I can't give you a short answer that addresses all possible
reasons for this variation in pleasure; that is the subject of my 255,000-word
book.
ER
doc too busy to make love to the woman he's dating?
Q: I started dating (if you can even call it that) an ER doc about a month
ago. He is always really tired or really busy -- works 14 shifts a month, but
what exactly is a "shift"? I know they're rotating shifts. I REALLY like this
guy and can't tell if he truly works a ton of hours or if he's just blowing me
off. I'm thinking "if you're too busy to f*ck me, you are TOO BUSY" but I'd like
to give him the benefit of the doubt. Should I continue to wait for his call or
move on?
A: An ER shift is typically anywhere from 8 to 12 hours. However, by the
time the doc completes his dictations, paperwork, and wraps up the care on his
patients, each shift may be prolonged a few hours — or it may not, depending on
how busy the shift was. Working 14 shifts per month may not seem like much, but
ER work can really sap one's energy. I've worked many jobs in my life, and
nothing — I mean NOTHING — was even a tenth as exhausting as ER work. I used to
mow lawns, primarily using a push mower. Trust me, you've never seen anyone mow
a lawn as fast as me. I souped up my mowers so they could still do a good job of
mowing even when pushed at a breakneck speed. In the blink of an eye, I could
turn the mower around and accelerate to my mowing pace (which was faster than
most people run). I'd do this all day long, seven days per week. Tiring? Just a
pleasant stiffness in my muscles at night. Compared to ER, it was like being on
vacation.
If you think I'm getting off-topic, just bear with me for a minute: I'm
giving you this background information so you can fully grasp what I'm about to
tell you. Physically, the most taxing job I had was when I worked for a guy
carrying building materials up a hill (he was building a home on a hill so steep
that no truck could ascend it, so he hired me to carry the boards from the base
of the hill, a few hundred feet to the top. The man was really a slavedriver,
insisting that I carry two thick sheets of plywood at a time up the hill. An
average man couldn't even pick up two such sheets of plywood, let alone carry
them hundreds of feet up a hill, and do that over and over again — building a
home requires umpteen tons of lumber. Was I tired afterward? A bit, but that job
was a walk in the park compared to being an ER doc.
I could regale you with tales of my other 18 jobs, but the take-home message is
the same: nothing is nearly as exhausting as being an ER doc. Obviously,
ER work isn't especially demanding from a physical standpoint: witness the
paunchy physiques of most ER docs. However, ER work is mentally taxing, and that
is far more onerous than physically demanding jobs. If you care to think about
this from an evolutionary perspective, humans evolved to tolerate prolonged
physical activity quite well, and also sporadic mental stress — like being
chased by a saber-toothed tiger. Our "fight-or-flight" response is great for
dealing with such periodic stresses, but it does a miserable job of coping with
mental stress that goes on and on and on . . . such as what ER doctors face.
It's been scientifically proven that humans and animals have a more difficult
time coping with stress when the stressor(s) are not under one's control. You
may think the ER doc is in control of the ER, but he isn't. He can't control how
many patients flood the ER at any one time. If the patient volume is
overwhelming, he can't prevent another dozen people from walking in the door,
all screaming for attention NOW. He can't control what his patients are like,
some of whom are so out-of-control that one such patient could sap all his time.
There are hundreds of factors that are not under the control of ER doctors, and
these stressors malignantly affect the docs. After all, they're human.
Most ER docs love to feel that they're tough and can handle anything.
Unfortunately, they can't evade biological reality. Protracted, severe stress
induces biochemical changes within the body that produces noticeable changes:
muscles atrophy a bit, and there's a bit more fat, especially on the trunk.
There are a dozen other changes, but you didn't tune in for a lecture on
endocrinology, so I'll cut to the chase and discuss how chronic stress impacts
libido. Briefly, it reduces it, primarily mediated by a fall in the testosterone
level.
Don't think that I'm writing all this to excuse the apparent sexual exhaustion
of your quasi-boyfriend. I'm not. I've worked full-time in one ER and part-time
in another ER while doing other jobs on the side, such as writing and inventing.
Even though I'm typically a high-energy person, sometimes I'd be so drained that
on my days off, all I'd want to do is sit in a chair and stare at the wall. I
had so much that I wanted to do, but I was so pooped that I couldn't muster the
energy . . . except when it came to sex. On those rare occasions when I had a
girlfriend, I was never "too tired."
My diagnosis? There's a problem here. Either the doc you're dating has a problem
with his libido, or he isn't attracted to you. Since he is dating you, I suspect
that he must be attracted. Ergo, there is likely a problem with his libido.
Working rotating shifts (in which the schedule changes from day to afternoon to
night shifts in a cyclic fashion) is a great way to wreak havoc on the body.
People who work the night shift typically live a few years less than average,
and people who work rotating shifts face even greater stress, because their body
never has a chance to adapt to the constantly changing schedules. Hence, it
isn't surprising that an ER doc working rotating shifts would manifest some
collateral damage.
Other than the stress of ER, there are countless factors that may impair
sexuality. I won't try to offer a definitive diagnosis for him over the
Internet, but I'd like to help. I know more about sex than Dr. Ruth. That
may seem like bragging, but it's true, I assure you. She knows the basics, but —
yawn — what doctor doesn't? Compared to what I know, she is still in
kindergarten. Therefore, I have a lot to offer, so I will send you a
complimentary copy of my book,
The Science of Sex: Enhancing Sexual Pleasure, Performance, Attraction, and
Desire, if you don't mind reading an e-book. Reading that book will give
you a lot to mull over, including some things you've certainly never considered.
If you think I'm just hyping the book (but why I'd do that to encourage someone
to accept a free copy is beyond me), I'm not. There isn't a doctor in the world
who knows more about sex than I do. I read every book I can get my hands on that
is even remotely similar to mine, because I believe in checking out my
competitors. Consequently, I've read countless books in this genre, and most are
laughably mickey-mouse and an utter waste of time. My book will have your head
spinning, and if the information in it can't turn your man into a sexual dynamo,
well, it's time to search for another man.
Woman upset over how beautiful women can live on Easy Street without lifting a
finger
Q: I admit it, I'm jealous of my sister. She is beautiful — slim,
fairly large breasts, a sexy belly, great legs and rear, gorgeous face, radiant
smile, flowing silky blond hair — you name it, she's got it. I'm no dog,
but if she's a "10" (and she probably is), I'm a 6 . . . maybe. I received
better grades in high school and college, yet she makes more than I do. A
lot more. That is what bugs me — men are willing to give her anything she
wants, whether it's in her career, or in her personal life. She knows
this, so she isn't very responsible at work. She often comes in late,
makes excuses why she has to leave early, takes long lunch breaks, etc., but
she's never been fired. She's never done anything for her boyfriends
(except you-know-what), not even given one a card, but they're always showering
gifts on her. Expensive stuff, too, like stereos, DVD machines, clothes,
skis and ski gear, vacations to Europe, and even a new car . . . a BMW,
nonetheless! I've received flowers twice in my life, and she sometimes
gets them twice per day.
It's obvious why she receives so many gifts. If she were ugly, her rich
boyfriends would be chasing someone else, not her. This burns me up,
because it is so unfair! I don't know what I expect from you. Maybe
I just wanted to vent (a woman's prerogative, you know), but I'm wondering . . .
hoping, really, if you could say something to make me feel better. Can
you? Angela
A: Yes. First, let me attest to the veracity of what you said.
The world is unfair: it rolls out the red carpet for beautiful
women. Anyone who doubts this should watch ABC TV's 20/20 exposé on
how people are influenced by beauty. This program showed hidden-camera
footage of two women applying for jobs at various businesses. They wore
identical clothes, and presented comparable educational backgrounds. One
woman was gorgeous, one was not. The gorgeous woman always got the
job, was offered more money, and told that company policy about
the duration of lunch breaks was flexible — apparently just for gorgeous
women, because the other woman wasn't told this. The interviewers seemed
overly eager to please the stunning applicant, and one went so far as to say
he'd do everything he could in the future to promote her. The sun, the
moon, and the stars . . . just because she's beautiful. It wasn't what she
said, either; most of her replies were monosyllabic. When you're
beautiful, that's apparently good enough.
One of the truisms attributed to Bill Gates is, "Life is not fair.
Get used to it." He should know, because if life
were fair, he wouldn't have become the richest man in the world by selling
buggy, exasperating, second-rate software that makes my life as an author,
doctor, and inventor more frustrating and less productive than it should be . .
. see, men can vent, too. In any case, while I think his pithy comment
about fairness is cruelly harsh, it aptly sums up the way the world is, and what
you should do about it. Neither I, nor you, nor anyone else, can do
anything to temper the boundless affinity that men have for beautiful women.
You realize how immutable this preference is, so you just want cheering up.
That I can do.
First, you can take comfort in the fact that if you're a "6," you're a fox
compared to some women. You might be a Plain Jane relative to your
ravishing sister, but some women would give a million dollars, if they had it,
if they could look as good as you.
Second, you can take comfort in the fact that beauty is often ephemeral.
With each passing decade, the prevalence of beauty in women drops significantly.
So, while your sister and similar women may now have the world at their feet,
they probably won't for long. When this loss of beauty hits, women who've
coasted through the early years of their lives on their looks often panic and
think, "Yikes, what now?" Unfortunately for women, the traits
that our culture defines as being attractive for women erode more quickly than
the attributes that define an attractive man. Hollywood executives, with
tens of millions of dollars at stake, have no qualms about casting a 50- or
60-year-old male as the leading man in a movie, but how often do they cast a
woman of similar age as the leading woman? They're usually in their
twenties or thirties.
Third, you can take comfort in the fact that there is some truth to the cliché
about how beautiful women often don't have as many other attributes as less
attractive women. The "beautiful
woman syndrome" doesn't affect every beautiful woman, but there is some
statistical merit in this stereotype. To tell you the truth, had I been
born a beautiful woman, I wouldn't have busted my butt in medical school and
spent years working on other things in my "spare time." Unfortunately, I
have to work for a living. I'm not averse to work, but if someone handed
me things on a silver platter, I'd take them. So would most people, I
suspect. You and I can't get away with this, but beautiful women can . . .
so they do it. People who win the lottery always collect the check.
Can you blame them?
Fourth, you can take comfort in the fact that no matter how beautiful, smart,
rich, or talented a person is, there is always someone who is even more gifted.
Most of those beautiful women who you think spend their waking lives nodding in
agreement as the world praises them aren't dwelling on how fantastic they are,
they're moaning the fact that some women are even more attractive.
I think people should stop and smell the roses, instead of wanting more, more,
more — whether it's looks, money, fame, or whatnot. What's the point in
having more, if getting it only means that you keep setting your sights a notch
higher?
Fifth, you can take comfort in the fact that a gorgeous woman never really knows
if the man who loves her does so because of her personality and mind, or just
because she is beautiful. This is similar to the uncertainty that plagues
rich men, who often wonder if it's them or their money
that is so attractive. As a doctor who was privy to the private lives of
thousands of patients, I know that true love sometimes exists, but it's not as
common as conditional love: "I'll love you if you're attractive," or "I'll
love you if you're successful."
Finally, you can take comfort in the fact that you're a better, more competent,
more deserving person than your level of success might otherwise suggest.
Conversely, gorgeous women are sometimes haunted by the fact that they aren't as
competent or deserving as their level of success seems to indicate. I
suppose some of the really vacuous babes out there suck up all the accolades,
gifts, and attention without giving it a second thought, but I think most
beauties have some nagging doubts about how great
they really are. Sans their stunning bodies, I think most of them are
honest enough, at least with themselves, to admit that their lives would be a
whole lot different if they weren't so attractive.
Feel better now?
Dating a woman, but sexually intimidated by her because she's a doctor
Q: I'm dating a woman who is an MD. Everything is great in our
relationship, except for one thing. I'm reluctant to have sex with her,
because I am quite frankly intimidated by her medical knowledge, especially as
it pertains to sex. She must know every intricate detail, and I have this
old-fashioned notion that the man should be more of an expert in this area.
Any advice? Scott
A: Yes. First, chill out. Second, learn at least the basics
about sexual anatomy. Doctors know the correct terminology, and they
sometimes assume that other smart people know as much as they do.
Sometimes they do, but sometimes they don't. If she mentions a certain
term during sex, it'd be better if you didn't need to ask, "Um, what's that?"
Third, take comfort in the fact that while docs possess an extensive knowledge
of sexual anatomy, disease, and reproduction, they usually don't know much more
than an ordinary person about how to
have sex. I suspect this is the cause of your concern. You may
imagine that your girlfriend is a sexual dynamo, brimming with arcane knowledge
taught only in cloistered medical schools where it is passed in hushed tones
from one generation to the next. That isn't likely. The medical
school that I attended emphasized sexual education, but what I learned there was
less than 1% of what I've learned on my own. Frankly, there is so much to
cram into four years of med school that there isn't time to dwell on any one
topic. Hence, your friend obviously knows the rudiments of sex, but she is
most likely not an expert. If you read
my book, you'll know countless things that she doesn't know, and likely has
never considered. For example, in medical school every student studies the
various types of nerve receptors, but they're too busy with other things to
contemplate how to use that knowledge so as to optimize sexual pleasure.
Years after medical school, nerve receptors are but a distant memory in the
minds of most physicians, and expecting them to connect the dots and apply that
shaky knowledge to some novel application is asking a lot. I do this, and
a lot more, in my book. If you read it, you'll have a phenomenal knowledge
of sex, and you can teach her hundreds of things. Have fun.
How did I learn so much?
Q: How did you become such
an expert on sex? Jill
A: It's probably not what you think — I'm no profligate Charlie
Sheen. How did I learn so much? To begin with, I graduated in the top 1% of my
class in medical school. So, compared to other doctors, I learned more about not
just sex, but also more about anatomy, physiology, biochemistry, nutrition,
pharmacology, endocrinology, neurology, urology, gynecology, histology, and
embryology — which are the underpinnings of knowledge about sex. Second, in
terms of sexual education per se, I attended a medical school that emphasized
sexual education more than most medical schools. Third, I've read extensively on
this subject, going far beyond the material presented in medical school — which
I consider to be merely introductory Sex Ed 101 stuff. Fourth, I excel not just
at memorization but also at integrating knowledge. To put this in colloquial
terms, I'm good at "putting it all together" or "connecting the dots."
Incidentally, I think that ability explains why I'm so creative. Fifth, I've
conducted novel research, from which I've garnered some groundbreaking
information. Sixth, I have a naturally curious mind. Everyone knows that sex
does not feel the same with different partners or even from time to time with
the same partner. I was intrigued by what accounts for this often remarkable
difference in pleasure, so I dug deep — very deep. In the process, I learned
some fascinating things.
Afraid of marrying a man who might become bald
Pezzi wonders, "Does she think that only men age?"
Q: How can I tell if a man will become bald? It'd be a nightmare for
me if I married some great guy, then he lost his hair . . . because my love for
him would go right out the window. I can't see myself ever being attracted
to someone who is bald, so I want some foolproof way of knowing in advance if
he'll keep all his hair. Can you help me, doc? Kristen
A: Yes. You need it. I have a number of answers and responses
to your question. In no particular order, they are:
1. First, all men and women lose hair as they age. Hair loss in
women is less apparent because they usually sustain a diminution of hair density
over the entire scalp, rather than in the discrete, progressive pattern that is
the hallmark of male pattern baldness. However, even in people who don't
"go bald," hair density decreases with age.
2. While everyone has the right to determine what they want in a partner,
I hope — for your sake — that you don't develop some of the maladies that plague
women when they age, such as wrinkles, cellulite, stretch marks, varicose veins,
sagging breasts, loss of breast size, a "tummy" that is refractory to sit-ups,
and excessive fat on the hips, thighs, and buttocks. Men can get fat, too,
but they're less apt to wrinkle, much less likely to have cellulite, stretch
marks, or varicosities, and almost immune from sagging breasts — for obvious
reasons. The scorecard? Presuming that a man keeps in shape, his one
major sign of aging is hair loss. Women face more risks, which may be why
our society thinks that older men can still be very attractive, but older women
are rarely coveted. If you disagree with this, don't kill the messenger.
I'm just relaying what is common knowledge.
3. Baldness actually complements the faces of some men. Take Dr.
Phil (of Oprah fame), or the actor who portrays Admiral Chegwidden on
JAG. I am not gay, or bisexual, but I can tell if a man is attractive
or not, and I think both men are handsome in spite of their baldness.
Furthermore, in my opinion, I think they'd look worse with more hair.
4. Baldness is now more treatable than ever, with hair transplants and
various anti-DHT meds and whatnot. The bad news about the anti-DHT drugs
is that while they may restore hair, they can decimate a man's sex life by
reducing his libido, impairing erectile performance, and inducing a very gradual
shrinkage of the penis. Any doc who is unaware of these risks is either
brain dead, inexperienced, or gullible enough to be hoodwinked by the
pharmaceutical industry. One of my pet peeves is stupid drugs ads.
One ad that I recall was when the maker of Propecia®
(finasteride, an anti-DHT drug) attempted to make men believe that taking
Propecia every day was something as innocuous as taking a daily "vitamin pill."
How ridiculous. Vitamins are essential for life and generally just
beneficial, while anti-DHT drugs have plusses and minuses. However dismal
it is to face the dilemma of choosing to benefit one's hairline at the risk of
impairing one's sex life, there is good news on the horizon. A doctor in
France discovered a way to clone a man's own hair cells, obviating the problems
of tissue rejection, and avoiding the quagmire of social issues that plagues
other cloning endeavors.
5. Keep in mind that one's perception of beauty changes with age.
When I was 15, I thought women aged 40 were antiques. Now that I'm that
age, I know some 40-ish women (all married, unfortunately for me) who are
mesmerizingly beautiful. I suspect that when I'm 60, women of that age
will look a lot better than they do now.
6. OK, to answer your question. There is no simple inheritance
pattern for baldness, as people sometimes believe. Many genes contribute
to this, so you cannot assume that a man will be bald just because his father or
grandfather was. My advice? If you love the man, marry him. In
twenty years, you'll probably be more worried about your own beauty problems
than his. Plus, as I mentioned above, medical science is nearing the time
when people can choose to have as much hair as they wish . . . or can afford (I
assume cloning won't be cheap). However, we haven't made comparable
progress in combating many of the beauty issues that women face.
Consequently, some day you might actually welcome some erosion of your partner's
attractiveness, because yours will surely erode, too. If his appearance
never waned, he'd probably eventually dump you and choose a younger partner.
Bottom line? I assume you think you either won't age, or that if you do, a
man shouldn't care how much you go to pot. Just hope your future husband
is a lot more forgiving of human imperfection than you are.
Phytoestrogen myth
Q: I heard a naturopathic doctor on television say that phytoestrogens can
be anti-estrogenic or pro-estrogenic, depending on what a woman's needs are. Is
what she said true? Anna
A: No. While it is true that phytoestrogens can either
increase or decrease a woman's overall estrogenic effect, phytoestrogens have no
way of knowing if a woman has just the right amount of estrogen, too much,
somewhat too little, or very little. How did this myth about "depending on what
a woman's needs are" get started? If a woman has an estrogen excess, adding
phytoestrogens can indeed reduce her overall estrogen effect via the process of
competitive inhibition, which I thoroughly explained in my book. If a woman has
very little estrogen, phytoestrogens can indeed increase her estrogen effect. So
far, so good for the naturopathic doc. Here's where her statement falls apart.
If a woman's estrogen level is good or somewhat less than is optimal, adding
phytoestrogens will reduce her overall estrogen effect, once again via
competitive inhibition. Consequently, the woman who originally had just the
right amount of estrogen now has less than she should, and the woman who had
somewhat too little estrogen now has a worse deficit. Did phytoestrogens
"balance" the needs of these last two women? Hardly. That's why I cringe
whenever I hear this "balancing" baloney. I don't know if that doc truly
believes it, or if she was just trying to simplify it enough to squeeze it in
the ten seconds that seems to be the limit for sound bites during media
interviews.
More semen, better orgasm?
Q: Is it true that if a man ejaculates more semen, his orgasm will be more
intense?
A: No. I don't know how that myth began. Perhaps it originated
from people who mistook cause and effect, and noticed that more intense orgasms
are sometimes associated with a greater volume of ejaculate. However, it
wasn't the extra ejaculate that
intensified the orgasm, it was the more intense orgasm that created stronger
contractions of the genitourinary tract, thereby expelling more semen.
A
one-hour orgasm?
Q: I've seen books and videos that speak of a one-hour orgasm. Is that
possible?
A: That is just marketing hype. Once they've drawn you in with the
hyperbole, they begin equivocating, saying something along the lines of, "It's
not really a one-hour orgasm, it's a prolonged period of heightened
awareness and pleasure." If that is the case, then I had a three-hour orgasm when I
was in fifth grade and I'd gawk for hours at a Ski-doo snowmobile catalog.
Heightened awareness? You bet. Pleasure? Ditto.
While some orgasms can be unusually prolonged, a one-hour orgasm is a
pipe dream. The reason for this is simple: orgasm involves the release of
neurotransmitters. The brain cannot store enough neurotransmitters to permit a
one-hour orgasm. Here is an analogy. Imagine that you pump water into a water
tower; that's like storing neurotransmitters in preparation for their eventual
release. Now imagine that you blast a hole in the side of the water tower, and
the water gushes out — that's analogous to the orgasm. There is a limit as to
how long the water will flow, because the water tower has a finite size.
Similarly, there is a limit to the duration of an orgasm, because the brain does
not have an infinite neurotransmitter supply. Some nutrients and drugs can "pump
up" the neurotransmitter stockpile to permit a longer and more intense orgasm
(as I explain in my book), but nothing currently known permits a one-hour
orgasm.
Status orgasmus is an orgasmic state lasting twenty seconds to one
minute. Having witnessed this, I can attest that the woman did indeed appear to
experience an unusually prolonged orgasm. However, I'm skeptical of women who
claim to have fifteen-minute orgasms. I think they experience a prolonged
preorgasmic sexual peak that feels very good, but does not deliver a
fifteen-minute period of true orgasmic pleasure.
Spot reduction/enlargement
Slimming thighs/enlarging breasts
Reducing cellulite
Q: In your book, you discuss how it is possible to enlarge the breasts
using a high-tech bra that actually modifies enzyme activity and blood flow.
Could this technique be used elsewhere in reverse? I want to reduce the
size of my legs, which are chubby in proportion to the rest of my body, which is
slim. I don't want liposuction for several reasons. First, I can't
afford it. Second, I'm afraid of the potential surgical complications.
Third, liposuction doesn't do much for cellulite. Since your technique
preferentially targets the outer fat, it seems to be an ideal way to reduce
cellulite.
A: Yes, that technique can be used in reverse for spot reduction and
treating cellulite, too. Spot reduction acquired a bad name because the
old recommendations were ineffective. For example, men were told to
exercise their oblique muscles to reduce the size of their love handles.
That just doesn't work. A man could have the strongest oblique muscles in
the world and still have love handles. While the old ways were
unsuccessful, this doesn't mean that spot reduction is impossible. Just
because man can't fly by jumping off a cliff and flapping some makeshift wings,
this doesn't mean that man cannot fly. Given the right tool — an airplane,
a rocket belt, or even a hang glider — flight is easy. The key is the
right tool. The same is true with spot reduction. With the right
device, it's possible to selectively slim or enlarge part of the body. I
discussed the science behind this concept in both
The Science of Sex and
Fascinating Health Secrets.
What can I do to climax during intercourse?
Q: What can I do so that I can climax during intercourse? I heard
that only one-third of women regularly climax during coitus, so I'm not alone. I
tried all the usual recommendations (such as more foreplay and the coital
alignment technique), but they did not help.
A: You might benefit from using testosterone or other drugs to improve
sexual sensitivity. Another possibility is using the Vag-TTS, which
enhances vaginal sensation. All of this is discussed in
The Science of Sex.
Increasing height: A good idea? Nuts?
Q: Hello Dr. Pezzi, about a week ago I stumbled across your site and
everyday I've been coming back for a few hours to read more. It is very
well put together and extremely entertaining. The sheer amount of
information you've shared with everyone is staggering. I've easily added
10 new bookmarks to my favorites list from your pages. So thank you.
:-)
Anyway, I'm a senior in high school,
and my question is this: I read your "What
Really Turns Women On" page, which
you separated into four categories:
Brains: I consider myself of above-average intelligence.
I do well in school, I ask a lot of questions, read a lot, etc.
Power/Wealth: I come from a fairly well-off family and
unless I manage to somehow majorly botch something up (which is always a
possibility, eek) odds are I'll be successful too. That's how it has been
for generations.
Fame: I'm working on that one.
:-)
Appearance: This is where my problem is. My body is in
good shape, and I'm very athletic. As far as facial features on a scale of
1 to 10, I'd probably give myself an 8. By no means am I going to be
appearing on the cover of any magazine, but I also won't turn a woman into stone
if she looks at me. I've always been a reasonably popular guy.
My problem is that I'm short. I'll be 18 at the end of November and
I'm only 5'4". Every male on my father's side of the family going back
many generations has been 6' - 6'3" or so, but my mom's side is relatively
short. I got the short end of the genetic stick on that one (pun intended
of course).
It's a problem though, and I'm embarrassed (even in e-mail) to ask about
it. I've spent more time than is probably healthy trying to find some
statistic somewhere that said it didn't matter, but everything I found said
things like "95% of women wouldn't date a guy shorter than them" and "97% of
women polled say their spouse must be taller than they are" — things like that.
And those blasted platform-esque shoes that are in style now only make it worse.
I've looked online and in the library, but I can only find web sites that
will "sell me the secret to growing taller for only $9.99 a month" and then spam
me with a dozen popups — those are sites I tend not to trust. I'd also
heard about a young woman who wanted to be an airline stewardess but she was too
short so she had some doctor crank apart her legs and thighs a tiny bit twice a
day to add a few inches leaving her bedridden (with multiple fractures in both
legs and thigh) for 9 months. The scary thing is I'd almost do the second,
so I figured I'd ask you. Is there any way you can improve height? I
know I'll never be 6'. I need to be realistic, but if there's a way to add
3 or 4 inches I'd be ecstatic.
Anyway, thank you for reading this far. This was a bit longer than
I'd intended and again, I know you're busy so if you can't respond I'll
understand completely.
Thanks, (name withheld by request).
A: At your age, the only way I know to add three or four inches of height
is via surgery. There are two ways of viewing whether it's nuts to consider such
an extreme option:
Yes, it's nuts: Even if 99.9% of the women turn their
noses up at you, to get married and have a successful life in terms of emotions
and love, it takes only one woman who adores you. Some women are short and
prefer a man who does not tower above them. That makes kissing, hugging,
and lovemaking more enjoyable. Even in women who aren't short, some don't
give a hoot about height. For example, one of the women in my "Beautiful
Women in the ER Contest" is exceptionally attractive, but she told me that a
man's physical attributes mean nothing to her. Want another example?
Years ago, I worked for a man whose birth defects left him with one of the
smallest, most deformed bodies I've ever
seen, yet he was married to a woman half his age who was very attractive in
every way (about 5'6", 115 pounds, pretty face, enticing breasts and legs, and a
great overall shape) . . . and no, he wasn't rich. His secret? He
had a dynamic personality, and did not feel handicapped by his handicaps.
Bottom line? You
could get married and not have to settle for the leftovers.
No, it's not nuts: Sure, it takes only one such woman
to fall in love with you . . . but good luck finding her. Even in men who
aren't short, finding a great match can be incredibly difficult. Since
most women do care about height, this problem will be compounded.
Apart from the romantic aspects, height is a major attribute in other areas,
too. Statistically speaking, taller men get better jobs and make more
money. If you've read some of the comments on this web site that I made
about appearance, you know that I think it's crazy how the world showers some
people with gifts just because they look a certain way. However much I
think it's nuts, most of the world evidently does not agree with me.
What may reduce vaginal tightness?
Q: Dear Sir: I am in need of help answering a question about my
wife's vaginal size. I'll be brief and to the point.
We have both been married before. My wife has three children.
Our sex life has been very good until now, nine years after marriage. Her
vagina is no longer tight enough for me to enjoy. She lost weight due to
dieting, and she is 51 years old. But the change in her vagina seems to
have developed suddenly.
I have always trusted my wife, but doubt has moved in because of this.
I am not very well endowed, and as most men I have always been bothered by that.
But my wife has made me feel secure, until now.
Please advise me as to the ways a woman's vagina can change, other than
childbirth and sexual intercourse. My wife is in good health and looks
great, and is on hormone therapy and is not experiencing many problems from the
change of life.
Your help is needed. Thanks, (name withheld by request)
A: First, let me assuage your apparent concern about the
possibility of your wife being unfaithful. It is very unlikely that her
reduced vaginal tightness is attributable to intercourse. Given the
scenario you presented, the most likely culprit is weight loss. Dieting
induces a loss of both fat and muscle. Muscle loss is more
pronounced when the diet is more extreme. When muscles are catabolized
(broken down) to provide energy, the muscles atrophy. This affects most
muscles in the body, including the muscles around the vagina. When they
atrophy, vagina tightness decreases.
In The Science of Sex,
I discussed weight loss because it is a subject that most people approach in the
wrong way, and because obesity affects sexuality. There is a correlation
between obesity and a number of diseases (such as heart disease, diabetes,
cancer, and arthritis) that can negatively affect sexual pleasure, performance,
and libido. I give numerous tips for achieving weight loss without
torturing your body or torturing yourself with hunger pangs. One of the
tips reveals how to lose weight without dieting, drugs, herbs, exercise, or
surgery. That may seem to be impossible and it may seem too good to be
true, but it works and it is not unpleasant. Somehow, this fact escaped
notice by the weight loss “experts," who recycle the same old tired advice year
after year. Surprisingly, some of these supposed experts are themselves
fat, which suggests that they are clueless. When I was an intern, I was so
fat that I could not see my feet when I stood up. Now, I am in good enough
shape to be an underwear model. Back in the days when I was a blimp, I
thought I'd never be able to lose weight. I grew fond of my doctor's
smock, which camouflaged the blubber fairly well. Eventually, I was so
disgusted by my potbelly that I decided to lose weight, and I did.
Painlessly. The key is knowing what to do.
OK, back to the subject of vaginal tightness. While dieting likely
triggered your wife's vaginal laxity, stopping the diet won't immediately
improve vaginal tone. It takes time for muscle to regenerate. This
process can be accelerated by performing Kegel exercises, which are discussed in
my book and myriad other sources. However, my book discusses Kegel
exercises and vaginal muscles in far more detail than you will find elsewhere.
Most of these discussions are trite, simplistic, and sometimes even laughable.
If you want an immediate improvement in vaginal tightness, your wife
could use a vaginal wedge or the Vag-TTS, both of which are discussed in my
book. You could also use a penile vacuum cylinder (colloquially termed a
"peter pump"). Correctly used, this device can produce slight to moderate
long-term enlargement and pronounced short-term enlargement (the latter effect
is accomplished via induction of penile edema). The edema is relatively
ephemeral, but it typically lasts a few hours — certainly long enough for
intercourse. The edema does almost nothing for penile length, but it can
dramatically increase diameter. Naturally, this increases subjective
vaginal tightness. For reasons that I explain in my book, tightness
improves more than size. Thus, when the penis is thicker, or the vaginal
diameter is decreased, tightness increases more than the change in size.
This may seem like Greek to you now, but the book makes it crystal clear.
The bottom line is that relatively small increases in penile diameter (or a
relatively small reduction in vaginal diameter) can produce a substantial
improvement in tightness. However, this works both ways, too. A
relatively small reduction in penile diameter (or a relatively small increase in
vaginal diameter) can substantially diminish tightness. Thus, it may be
that your wife's vagina isn't much larger than before. She may be just a
bit larger, but this may seem like a big change because of the disproportionate
variation in tightness with changes in size.
If she was near the threshold at which a small change in size produces a big
change in tightness, you could easily interpret her vaginal looseness as
developing "suddenly," as you mentioned.
Some medical problems can affect vaginal tightness, such as Cushing's
disease, some neurological diseases, and diseases that induce cachexia
(wasting), such as certain cancers and AIDS. Several medications can
affect vaginal tightness by causing muscle atrophy or reducing muscle tone.
Simple aging is usually associated with loss of musculature, and this atrophy is
accentuated if testosterone is deficient (as it so often is). Other
hormonal problems (such as thyroid disorders) affect muscle strength, and this
can manifest as reduced vaginal tightness. Hormone replacement therapy can
itself affect vaginal tightness unless both estrogen and testosterone are given.
Typically, women receive estrogen only. While this is better for the
vagina than receiving nothing, replacing estrogen but not testosterone increases
production of a transport protein (sex hormone binding globulin, or SHBG) that
binds to, and inactivates, testosterone. This lowers the bioavailable
testosterone level, and can exacerbate a testosterone deficiency. This can
accelerate muscle loss (thus decreasing vaginal tightness) in addition to
affecting bone density, mood, sleep, confidence, certain aspects of
intelligence, libido, and other things. The route by which hormones are
administered (oral, transdermal patch, etc.) affects SHBG production. I
discuss these subjects, and hundreds more, in further detail in The Science
of Sex.
Is
love a social construct or sexual attraction?
Q: Dear Doctor,
I am doing a term paper on love. My question is: "Is love a social
construct or sexual attraction?"
Paul
A: Neither. Marriage is a social construct. Love is
much more instinctive. If you were born into a world in which marriage did
not exist, there is a good chance that you would never conceive of that
construct. If you doubt me, think of the millions of people who did just
that.
Love is not a social construct. It has tangible roots in our
biology. Definable changes in hormones and brain neurotransmitters occur
when a person is in love, or is on the path leading to it. This is
discussed in The Alchemy of Love and Lust: How Our Sex Hormones Influence Our
Relationships by Theresa L. Crenshaw, MD, and to a lesser extent in my book
(The Science of Sex).
Love is also not sexual attraction. Sexual attraction is one of the
key ingredients that spark feelings of love, but sexual attraction per se is not
love, nor anything even close to it. Offhand, the most attractive woman I
can think of is Helene Eksterowicz from the second The Bachelor
miniseries. Am I attracted to her? How could any red-blooded man not
be attracted to her? On the day that looks were handed out, she won the
lottery. But do I love her? No. Lust is essentially a synonym
for sexual attraction, but love is not.
So what is love? Rather than discuss this from a hormonal/neurochemical
perspective, I will address it in shirtsleeve English. Love develops when
the following three conditions are met:
1. There is attraction. This is usually predicated on physical
attraction, but sometimes on an appreciation of brainpower, talent, personality,
financial resources (think Melinda Gates), social status (think of the women who
went gaga over President Clinton), or fame.
2. The feeling is reciprocated to some extent.
3. And, most importantly, a little voice in your head tells you that this
is the best person you can hope to get at the current time.
This latter point is key. I could be attracted to many women, and
some of them could be attracted to me, but I would not fall in love with someone
if I thought I could get a better catch. Incidentally, this "best catch"
requirement explains why people usually fall in love with ONE person, since
there is just one best catch.
It is interesting to consider how self-perception narrows the field of
candidates for love. This is all the more interesting when you realize
that self-perception influences not just this nebulous thing called love, but
also hormones and neurotransmitters. What is so intriguing about this is
that when self-perception is less, the field of potential (not
necessarily likely) candidates widens. A man who is a "5" (and
views himself as such) could be attracted to women whose appearance is average,
above-average, or beautiful. Assuming his interest was reciprocated, that
man could potentially fall in love with any one of millions of women, ranging
from a Plain Jane living next door, to Helene Eksterowicz. However, if
that man were a "10" and realized it, he would likely turn up his nose at less
attractive women — even 7's and 8's that most men would be thrilled to have a
relationship with.
Get yourself a cup of coffee, sit down, put your feet up, and ponder this
matter for a while. It has broad implications for contentment, happiness,
and targets that you set for what you want to get out of life.
Some causes of diminished libido
Q: I am a 26-year-old woman and my partner is 32. We have been
together for five months and last month decided to get married. Yet I have
problems with him in terms of sex. At the beginning of our relationship,
he was horny. A month later he began to lose interest in sex. We
started to do it less often (like once in ten days). When I talked to him about
my worries, he told me that he had this problem in his past relationships.
He also revealed that his fiancée left him because they were having sex only
once per month. He has been seeing a therapist for the past three months.
This doctor gave him an antidepressant as a part of therapy. Since then he
cannot come at all. He does it only for my pleasure, I guess. We
have sex once every seven to ten days. This depresses me a lot. What
do you recommend? Is there any hope? Should I be patient? How
should I behave? Thank you.
A: This matter is obviously troubling to you, and for good reason.
At your age, you should be having the time of your life in the bedroom. If
things are bad now, and they are, they will only get worse in the future unless
he is treated. Being patient and waiting will do no good. Based on
what you said, there is no indication that this problem will spontaneously
resolve.
Fortunately, loss of libido is almost always correctable. I don't
know if doctors in your country at adept at treating it, but if they aren't,
either you, your fiancé, or his doctor should read my book (The
Science of Sex) for information on how to proceed. Given that his
doctor prescribed an antidepressant which worsened his problem, I doubt that his
physician is knowledgeable about sex — or if he is, your fiancé is not telling
him about his sexual difficulty. Some antidepressants interfere with
sexuality, but one increases libido and orgasmic potential (I discuss this in my
book).
However, changing his antidepressant is not the sole solution to this
problem since his difficulty with libido preceded antidepressant use. As a
doctor, I am concerned that he might have some medical problem that is lowering
his testosterone level (testosterone is the primary hormone governing libido in
both sexes). Testosterone production can be reduced by testicular trauma,
radiation, chemotherapy, or tumors. Orchitis (testicular inflammation) can
also lower testosterone levels; this may occur in men who develop mumps after
puberty. Pituitary tumors and AIDS can decrease testosterone levels, too.
Men may have low testosterone as a result of some genetic diseases, such as
Kallmann’s syndrome, Klinefelter’s syndrome, Prader-Willi syndrome, or myotonic
dystrophy, the most common form of muscular dystrophy in adults.
Testosterone levels can fall because of stress, long-term exposure to cigarette
smoke, excessive alcohol consumption, obesity, sleep deprivation, sleep apnea,
overtraining, and a diet that is excessively deficient in protein, fat,
calories, potassium, or zinc. Phytoestrogens, xenoestrogens, and exogenous
estrogens can also reduce testosterone output. Exposure to cadmium can
reduce libido, too. Here is an excerpt from my book:
Cadmium is a toxic metal that can partially
block the action of zinc in the body. Thus, even if your intake and absorption
of zinc are adequate, you may be functionally deficient in zinc if you have
ingested or inhaled cadmium, which functions as an anti-nutrient. Everyone has
been exposed to cadmium in food (particularly shellfish[1]),
water, and air, but cadmium levels vary considerably depending on your
occupation, location, and other factors. Cadmium is present in rechargeable
nickel-cadmium batteries, pigments, polyvinylchloride (PVC) stabilizers, and
some metal coatings, paints, inks, ceramics, and glass. Cadmium can also be
found in other metals as an impurity, and in some fertilizers, nematocides[2],
pesticides, and fungicides. Burning coal, oil, gas, or wood can release cadmium,
as can soldering, welding, smelting, and waste incineration. The latter need not
be on an industrial scale; even a neighbor burning trash might send cadmium
wafting into your yard. Incidentally, cadmium is most easily absorbed through
the lungs.
Here are some more facts you should know about cadmium:
· Cadmium is widely distributed throughout the body, but it accumulates
primarily in the kidneys and liver of humans and animals. It is inadvisable to
eat liver or kidneys since there is no practical way for you to know the cadmium
content of those foods.
· Cadmium is present in cigarette smoke. The cadmium level in people who
smoke is substantially higher than in nonsmokers.
· Galvanized water pipes can significantly increase cadmium levels in
drinking water.
· Oysters are reputed to be an aphrodisiac (perhaps because of their zinc
content), but they are often contaminated with cadmium and hence may hurt your
sex life.
· In experimental animals, low dietary levels of calcium, iron, or zinc
increase cadmium absorption.
· Cadmium can be released from nickel-cadmium batteries if they are put
in backwards, crushed or otherwise damaged, burned or subjected to a short
circuit, or even just overheated. According to a representative of the Eveready
Battery Company, nickel-cadmium batteries can release cadmium at temperatures as
low as 113° F[3]. Since batteries heat up when they
are used or recharged, the ambient temperature need not exceed 113° F for
cadmium emission to occur.
And here are a few tips for doctors:
· Since cadmium has a long persistence in the body (its elimination
half-life is 20 to 30 years), you cannot count on the passage of time to reduce
cadmium levels. Since cadmium is so easy to acquire and so difficult to get rid
of, older people generally have higher cadmium levels.
· Chemet®, also known as succimer or dimercaptosuccinic acid (DMSA), is a
chelator that can remove cadmium from the body.
· Blood levels show recent exposure to cadmium, while urine levels show
both recent and long-term exposure.
· An early sign of cadmium-induced nephropathy is increased proteinuria,
especially beta-2-microglobulin.
--------------------------------------------------------------------------------
[1] To minimize cadmium ingestion from eating
shrimp, choose farm-raised shrimp. Some Midwest farmers, fed up with the
vagaries of raising traditional crops and animals, now grow shrimp in ponds in
their fields.
[2] Nematocides are substances that kill nematodes (a.k.a., roundworms),
such as hookworms or pinworms.
[3] As a longtime electronics enthusiast, I was skeptical that cadmium
emission could occur at such a comparatively low temperature. However, the
Eveready representative insisted that was true, adding, “That’s one of the
reasons we stopped making nickel-cadmium batteries.”
-----------------------------------------------------------------------------------------------------------------------------
My book contains much more information on ways to enhance libido, sexual
pleasure, orgasmic ability, and sexual performance.
She is attracted to her doctor — how should she proceed?
Q: I was attracted to my doctor the first time I met him. I have
never before had this kind of instant attraction to any man. I think I
like him so much because I really go for smart men with a compassionate side.
While I am normally shy, I have managed to flirt with him a little bit. He
kids with me and seems not to mind my flirting.
I guess my concern is that what I see as possible interest on his part
could just be a great bedside manner. Maybe he is naturally nice to all
his patients.
A: That is possible. I've had women misread my pleasantness,
too. Some of these situations were so memorable that I will include them
in my next book of ER stories.
Q: This would be so much easier if he were my cable guy
or someone I met in a grocery store! I have so little experience in
flirting and reading men for positive signals because they will approach me
first. How can I tell if he really is interested? Is there anything
I can do or say to let him know I want to get to know him?
By the way, I'm being treated for anemia, so it's not like I have some
scary disease that would be a turn-off. Thanks. Judy
A: This is definitely a touchy situation. On one hand, you
don't want to create an uncomfortable situation if he is not attracted to you.
On the other hand, you don't want to pass up an opportunity for a potentially
great relationship.
I assume he is not married, but he may already be involved with someone,
unbeknownst to you. Assuming that he is available and attracted to you, he
still may not want to become involved. Why? State medical boards
frown on doctors becoming sexually involved with patients. I exhaustively
researched this matter a few years ago when another reader asked me a similar
question. From what I determined, the only relatively safe course of
action is for the doctor to terminate his professional relationship before he
becomes personally involved. I said "relatively safe" because there is
always the potential for you to raise a stink with the medical board, regardless
of when he last saw you as a patient, if things don't work out and he ends the
relationship. You strike me as someone who is not likely to do this, but
some woman, somewhere, gave credence to the phrase "hell hath no fury like a
woman scorned." In fairness to women, rejected men can be equally
malevolent.
I think the most logical way to proceed is to:
1. Determine if he is available.
2. If he is available, determine if he is willing to risk dating a
patient who is agreeable to becoming an ex-patient.
3. If he is willing to date an ex-patient, determine if he is interested
in you.
You can do this on your own, of course, but it may be a delicate situation, as I
discussed above. If you want, I will intercede on your behalf if you give
me his name and e-mail address (I won't tell him your name). Thus, if he
is involved with someone, or not willing to date a former patient, then you
needn't go through the uncomfortable situation of telling him that you are
interested.
PS: You've heard of the FOX network's Married By America?
Well, this is Married By www.ERbook.net!
:-)
PS #2: I just had another thought about your statement, "Is there anything
I can do or say to let him know I want to get to know him?" Yes, there is.
If you want to handle this matter on your own, you could look him in the eye,
pause for effect, and then say, "I like you." If he pats you on the
shoulder, gives you a perfunctory brief smile, says "I like you, too, Judy,"
then resumes from where he left off, it is a safe bet he is not personally
interested in you. On the other hand, if he stops dead in his tracks and
looks stunned, that is because he is searching for a way of letting you know he
is interested, without doing something that might run afoul of the state medical
board.
Reader heard a rumor . . . is it true?
Q: Dr. Pezzi: I think that your website is quite entertaining and
informative at the same time. I enjoy it very much. I am a
19-year-old college student and I have a question regarding something that my
friend heard somewhere. He said something about a correlation between
sexual pleasure and the size of a woman's posterior. More specifically
that a woman with a bigger ass will derive more sexual pleasure from sexual
activities than one with a smaller ass. Is there any truth to this?
Jared
A: I consulted several female friends, including ones with slim behinds
and others with steatopygic derrières (steatopygia = an extreme accumulation of
fat on the buttocks), but the latter ones were too busy moaning to answer my
question. OK, I'll be serious. There is no truth to this rumor.
If anything, the converse is true. Women with more testosterone are likely
to have smaller buttocks, and also a better sex life because testosterone
enhances libido and heightens sexual pleasure.
Enlarged
labia minora cause for concern?
I receive a surprising amount of e-mail from women who remain virgins because
they're embarrassed about what they think are enlarged labia minora (the thin
hairless inner lips that surround the vaginal opening, in contrast to the labia
majora, which are the larger, fatty, hair-covered outer lips).
If you are one of those women, relax! Men often think that large labia
minora are sexy and desirable, so what you have is a definite plus, not
something to be ashamed of. I've performed thousands of pelvic exams, and
I've yet to see any labia minora that are too large. Nor have I seen
excessively large labia minora in textbooks. What you're worrying about
simply doesn't exist.
If you're thinking about surgery to reduce their size, forget it. Why
would you incur pain, possible numbness, and the other risks of surgery (not to
mention its cost!) to lop off something that men adore?
A woman who read the above explanation still wasn't convinced, and she wrote to
say that I was minimizing the problem just to make women feel better. Not
so. I'm not one of those doctors who feels a need to assuage the anxieties
of my patients even when they have reason to be anxious. If I thought
large labia minora were a problem, I'd say so.
Copyright © 1991 - 2006 by Kevin Pezzi, M.D.
All rights reserved. No liability is assumed with respect to the use of
the information herein. You should consult with, and obtain the approval
of, your personal physician before instituting any of the measures presented.
No material intended for the general population can attempt to treat specific
individuals, and no material in this web site should be construed as offering
individual medical advice. Given the innate variability of people, it is
critical that your physician approves the adoption of any information herein
contained as being safe and effective for you. A physician's
circumspection is his—and your—greatest asset.

Reset counter 10-31-2003/Created 8-19-2001
|